12
Jun
Elderly Fall Statistics: Nursing Home, Hospital & Patient Safety Data Report
2026 Elderly Fall Statistics: Nursing Home, Hospital & Patient Safety Data Report
Falls remain one of the most significant patient safety challenges affecting older adults in the United States. As the aging population grows, elderly fall statistics continue to show a major burden across emergency departments, hospitals, nursing homes, long-term care facilities, homecare settings, and family caregiving environments.
A fall can begin as a single event, but the outcome may affect nearly every part of a senior's health journey. Fall-related injuries can lead to emergency department visits, hospitalizations, fractures, traumatic brain injuries, rehabilitation stays, reduced mobility, loss of independence, and increased long-term care needs.
Why Elderly Falls Are a National Patient Safety Issue
Elderly falls are not only a home safety concern. They are a public health, healthcare quality, and care-delivery issue affecting families, hospitals, skilled nursing facilities, assisted living communities, rehabilitation providers, and caregivers.
The same risk factors that increase fall injuries — weakness, balance decline, medication side effects, unsafe walking conditions, improper transfers, and reduced mobility — also increase pressure on emergency care, hospital systems, long-term care providers, and family caregivers.
Fall injuries increase emergency care use, hospital admissions, rehabilitation demand, and long-term care needs.
Nursing home fall statistics are closely tied to mobility decline, frailty, medication use, staffing pressure, and transfer safety.
At home, falls can increase family caregiving responsibilities, fear of walking, unsafe transfers, and loss of independence.
Report focus: elderly fall statistics, nursing home fall statistics, patient fall statistics, hospital fall data, patient safety statistics, caregiver injury trends, economic impact findings, and fall prevention statistics for elderly adults.
Related Data Areas in This Report
The Scale of Elderly Falls in the United States
National elderly fall statistics show that falls are one of the most common and costly patient safety events affecting adults age 65 and older. The numbers are important because a single fall can lead to emergency care, hospitalization, rehabilitation, reduced independence, repeat fall risk, and long-term caregiver burden.
For families, hospitals, nursing homes, discharge planners, and homecare providers, these patient fall statistics help explain why fall prevention remains a major public health priority.
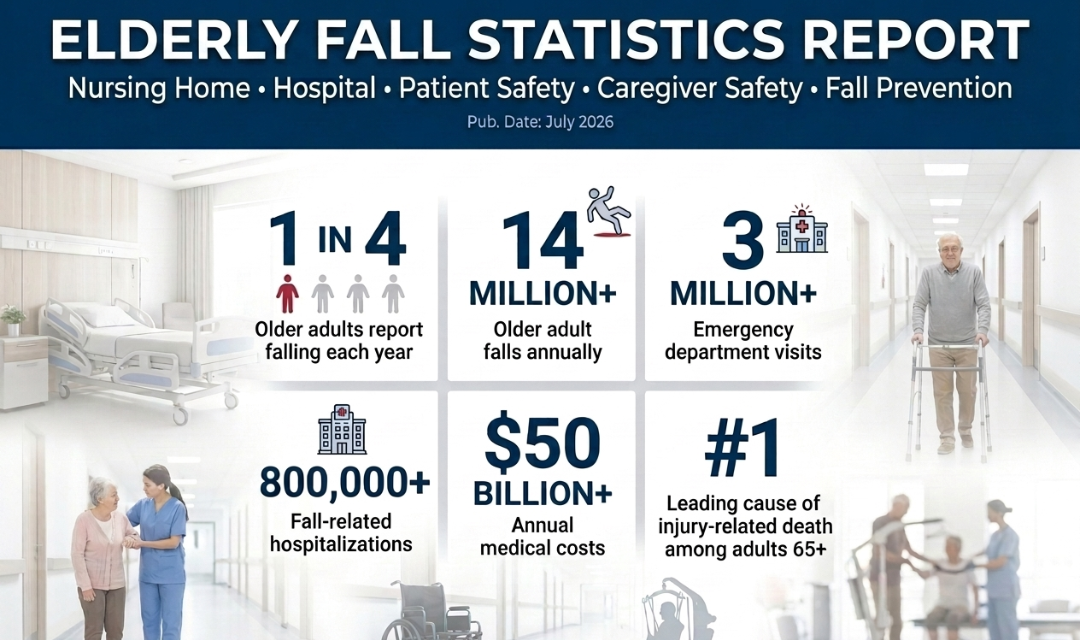
CDC data shows that more than one out of four older adults falls annually.
More than 14 million adults age 65 and older report a fall every year.
CDC reports that about 37% of older adults who fall report an injury requiring medical treatment or activity restriction.
CDC estimates approximately 9 million fall injuries among older adults based on reported injury data.
CDC fall prevention data reports about 3 million emergency department visits for older adult falls each year.
CDC reports about 1 million fall-related hospitalizations among older adults each year.

Why These Numbers Matter
Elderly falls affect emergency departments, hospital capacity, rehabilitation demand, nursing home safety programs, family caregiving needs, and long-term healthcare costs. The most important pattern is that many falls are preventable when risk factors are identified early and safer care environments are created.
Fall-related emergency visits and hospitalizations place pressure on emergency care, inpatient teams, rehabilitation, and discharge planning.
A fall can reduce independence, increase fear of walking, limit daily activity, and create new caregiving responsibilities.
National fall trends also appear in nursing homes and assisted living settings where frailty and transfer needs increase exposure.
Repeat fall risk makes prevention urgent after the first fall, especially when weakness, balance difficulty, medication changes, or home hazards are present.
Key Findings From National Elderly Fall Statistics
- Falls are extremely common: more than one in four older adults reports falling each year.
- The national burden is large: more than 14 million older adults report falls annually.
- Injuries are common after falls: about 37% of older adults who fall report a fall injury requiring medical treatment or activity restriction.
- Emergency and hospital burden is significant: older adult falls account for about 3 million emergency department visits and about 1 million hospitalizations each year.
- Falls are a patient safety issue: consequences include injury, hospitalization, rehabilitation, caregiver strain, and preventable loss of independence.
Related Data Areas in This Report
Nursing Home & Long-Term Care Fall Statistics
Nursing home fall statistics require a different level of attention than general elderly fall statistics because long-term care residents often have multiple overlapping risk factors. Frailty, reduced mobility, chronic illness, cognitive impairment, medication use, nighttime bathroom needs, and transfer assistance all increase the likelihood that a fall may occur.
Falls in nursing homes, assisted living communities, skilled nursing facilities, and rehabilitation centers are not only resident safety concerns. They are also patient safety statistics that affect care planning, staffing workflows, post-fall monitoring, quality improvement programs, and family trust in long-term care environments.
Why Long-Term Care Residents Face Higher Fall Risk
Many residents need help with standing, walking, toileting, bathing, transferring, or repositioning. When mobility decline combines with environmental hazards, staffing pressure, confusion, or medication side effects, a routine movement can quickly become a serious fall-risk event.
AHRQ notes that 30% to 40% of nursing facility residents who fall will fall again, making post-fall response and prevention planning critical.
Long-term care fall prevention requires investigation, monitoring, assessment, care-plan updates, and staff follow-through after a resident fall.
Bed-to-chair, wheelchair, toileting, and bathing transfers are common moments where balance, strength, and caregiver assistance matter.
Lighting, clutter, flooring, bathroom access, hallway layout, and bedside setup can all contribute to preventable long-term care falls.

Bathrooms combine slippery surfaces, tight spaces, urgency, poor lighting, and frequent transfer needs.
Nighttime movement can involve confusion, low visibility, fatigue, toileting urgency, and reduced staff observation.
Residents may attempt to rise unassisted, reach for objects, transfer too quickly, or misjudge their balance.
Unsafe pivoting, unlocked wheels, poor positioning, weakness, or lack of assistance can raise fall risk.
Long walking distances, clutter, poor footwear, balance problems, and fatigue can increase hallway fall exposure.
Resident-Level Risk Factors
Long-term care residents often have higher baseline fall risk because they may live with muscle weakness, poor balance, arthritis, dementia, stroke history, Parkinson's disease, vision problems, pain, incontinence, or multiple chronic conditions.
Medication side effects can also increase risk by contributing to dizziness, sedation, blood pressure changes, confusion, urgency, or slower reaction time. These factors often overlap, which is why fall prevention in nursing homes requires individualized assessment rather than a one-size-fits-all checklist.
Facility-Level Safety Challenges
Skilled nursing facilities, assisted living communities, and rehabilitation settings must manage fall risk while also supporting resident independence, therapy participation, toileting schedules, transfers, and daily mobility.
Staffing shortages, high resident acuity, inconsistent transfer assistance, poor environmental setup, and delayed post-fall follow-up can all increase the chance of repeat falls or preventable injury.
Key Findings for Nursing Home & Long-Term Care Fall Risk
- Falls are a major long-term care safety issue: they are among the most common adverse events discussed in nursing home and facility safety programs.
- Repeat falls require immediate attention: AHRQ reports that 30% to 40% of residents who fall will fall again.
- Transfer-related risk is central: bedside, wheelchair, toileting, and bathing transfers often combine weakness, balance difficulty, and caregiver assistance needs.
- Fall prevention is both clinical and operational: resident assessment, staffing, environment, equipment access, lighting, footwear, and care-plan updates all matter.
- Long-term care fall prevention supports patient safety: preventing falls can reduce injury, hospitalization risk, family concern, caregiver strain, and avoidable care escalation.
Related Data Areas in This Report
Hospital Falls, Readmissions & Patient Safety Statistics
Hospital fall statistics are a major part of patient safety reporting because inpatient falls can lead to injury, delayed recovery, extended length of stay, rehabilitation setbacks, discharge complications, and higher care needs after hospitalization. Unlike general elderly fall statistics, hospital falls occur inside a monitored healthcare environment, which makes prevention, documentation, and quality improvement especially important.
Falls remain a key hospital quality metric because they are connected to hospital-acquired injuries, nursing workflows, medication review, delirium prevention, mobility support, assistive device use, discharge planning, and readmission risk. For older adults, post-surgical patients, and patients with limited mobility, even a non-injury fall can create fear, functional decline, and loss of confidence during recovery.
Why Hospital Falls Are a Patient Safety Metric
AHRQ PSNet identifies falls as a common complication of hospital and long-term care settings, especially among older adults. Hospital fall prevention requires individualized risk assessment, multidisciplinary responsibility, safer environments, medication review, mobility support, post-fall review, and a culture that treats falls as preventable patient safety events.
AHRQ estimates that 700,000 to 1 million hospitalized patients fall each year.
Hospital fall rates are commonly reported at approximately 3 to 5 falls per 1,000 bed-days.
AHRQ PSNet reports that more than one-third of in-hospital falls result in injury.
Death or serious injury from a fall in a healthcare facility is treated as a serious reportable safety event.

Hospital patients may fall while getting out of bed, walking to the bathroom, reaching for items, or attempting to move without assistance.
Pain, weakness, anesthesia effects, medication changes, IV lines, and mobility restrictions can increase fall exposure after surgery.
Fall-related injuries can delay mobility recovery, increase therapy needs, extend hospitalization, or change discharge destination.
Falls after discharge may lead to emergency visits, complications, family concern, and possible hospital readmission.
Hospital-Acquired Injuries & Recovery Impact
Hospital falls can result in fractures, head trauma, soft tissue injuries, fear of walking, reduced activity, and loss of confidence. For older adults, these outcomes can interrupt rehabilitation, slow recovery, and increase dependence on staff, family members, or post-acute care providers.
Patient fall statistics also matter because falls can occur during routine activities such as toileting, transferring, ambulation, and bedside movement. That makes fall prevention a clinical, operational, and environmental safety priority.
Discharge Safety & Transitional Care Challenges
The risk does not end when a patient leaves the hospital. Discharge failures, poor home setup, lack of caregiver education, incorrect assistive device use, medication side effects, and unresolved weakness can all increase fall risk after discharge.
Strong transitional care planning can help reduce preventable post-hospital falls by identifying mobility needs, reviewing medications, assessing home hazards, arranging support, and making sure patients understand safe movement after hospitalization.
Key Findings for Hospital Falls & Patient Safety
- Hospital falls are common: AHRQ estimates that 700,000 to 1 million hospitalized patients fall each year.
- Fall rates are tracked as a quality metric: hospital falls are commonly measured per 1,000 patient bed-days.
- Injuries are clinically significant: more than one-third of in-hospital falls result in injury, including serious injuries such as fractures and head trauma.
- Falls affect recovery: inpatient falls can delay rehabilitation, increase care needs, and complicate discharge planning.
- Prevention requires a system approach: risk assessment, staff education, mobility planning, medication review, environmental safety, and post-fall review all matter.
Related Data Areas in This Report
Mobility Decline, Aging & Fall Risk Factors
Elderly fall statistics become easier to understand when the underlying fall risk factors are clearly identified. Most falls are not caused by one single issue. They usually happen when multiple health, mobility, medication, vision, environmental, and behavioral risks overlap at the same time.
For older adults, mobility decline can develop gradually through muscle weakness, balance changes, arthritis, chronic disease, stroke recovery, Parkinson's disease, dementia, sedentary lifestyle, poor footwear, foot pain, vision impairment, medication side effects, and home hazards. These risk factors affect patient fall statistics across homes, hospitals, nursing homes, assisted living communities, and rehabilitation settings.
Why Fall Risk Often Builds Over Time
Fall risk usually increases when strength, balance, vision, reaction time, confidence, and safe movement patterns decline together. A person may still be able to walk, stand, or transfer, but the safety margin becomes smaller.
This is why fall prevention statistics for elderly adults must be interpreted together with mobility decline, chronic health conditions, home safety, medication review, and caregiver support.
The CDC notes that most falls are caused by a combination of risk factors, and risk increases as the number of factors rises.
Poor strength and balance are major modifiable risks that can be addressed through screening, exercise, therapy, and safer mobility planning.
Medicines that cause dizziness, sedation, confusion, or blood pressure changes can increase fall risk in older adults.
After a fall, some older adults reduce daily activity. Less activity can lead to weakness, which can further increase fall risk.

Reduced lower body strength makes standing, walking, stair use, transfers, and recovery from a stumble more difficult.
Balance changes increase the chance of losing stability during turns, bathroom trips, uneven surfaces, or transfers.
Poor vision can make it harder to identify steps, clutter, cords, floor changes, furniture edges, and nighttime hazards.
Sedation, dizziness, confusion, and blood pressure changes can raise patient fall risk, especially after medication changes.
Joint pain, stiffness, and limited range of motion can affect walking speed, posture, transfers, and safe movement.
Neurological conditions can affect gait, coordination, posture, freezing episodes, weakness, and reaction time.
Cognitive changes can increase unsafe wandering, poor judgment, nighttime disorientation, and unassisted movement.
Loose rugs, poor lighting, clutter, slippery bathrooms, missing grab bars, and unsafe footwear can contribute to preventable falls.
How Mobility Decline Changes Daily Fall Risk
Mobility decline can make ordinary activities more dangerous. Getting out of bed, walking to the bathroom, standing from a chair, reaching for an item, stepping into a shower, or transferring from a wheelchair can become higher-risk movements when strength, balance, or coordination decreases.
This is especially important in patient safety statistics because many falls happen during routine activities, not extreme events. The goal is to identify risk before a fall causes injury, hospitalization, or long-term loss of independence.
Why Screening and Prevention Must Be Individualized
Two older adults can have very different fall risks even if they are the same age. One person may struggle with balance and foot pain, while another may have medication-related dizziness, vision impairment, or cognitive decline.
Strong fall prevention programs look at the whole picture: medical history, walking ability, transfer safety, medications, home hazards, footwear, lighting, bathroom safety, assistive device fit, caregiver support, and recent falls.
Helpful MedCare Mobility Resources
For readers comparing safe mobility options, homecare support, or assistive walking devices, these educational resources provide additional guidance without replacing medical advice or fall-risk screening from a healthcare professional.
Key Findings for Mobility Decline & Fall Risk Factors
- Falls usually involve multiple risks: weakness, balance decline, medication effects, vision problems, chronic disease, and home hazards often overlap.
- Mobility decline changes routine activities: walking, bathing, toileting, transferring, and getting out of bed can become higher-risk movements.
- Medical conditions matter: arthritis, Parkinson's disease, stroke, dementia, chronic pain, and sedentary lifestyle can all increase fall exposure.
- Fear of falling can worsen risk: reduced activity after a fall can lead to weakness, lower confidence, and further mobility decline.
- Fall prevention should be personalized: risk screening, medication review, safe home setup, appropriate mobility support, and caregiver education work best when matched to the person's needs.
Related Data Areas in This Report
Caregiver Injuries & Unsafe Patient Transfers
Caregiver injuries are an important part of patient safety statistics because unsafe lifting, repositioning, and patient transfers can create risk for both the caregiver and the person receiving care. When a caregiver is strained, rushed, fatigued, or unsupported, the chance of unsafe transfers, transfer-related falls, and delayed assistance can increase.
OSHA identifies manual patient handling as a major healthcare worker safety issue, especially for nursing assistants and caregivers who repeatedly help patients move between beds, chairs, wheelchairs, toilets, showers, and standing positions. These risks are closely connected to elderly fall statistics, nursing home fall statistics, hospital fall data, and long-term care safety programs.
Caregiver Safety Is Patient Safety
Safe patient handling protects more than the worker's back. It supports safer transfers, better mobility assistance, fewer rushed movements, stronger care continuity, and reduced risk during high-exposure moments such as toileting, bathing, repositioning, bed-to-chair transfers, and wheelchair transfers.
OSHA cites BLS data showing 18,090 musculoskeletal disorder cases involving days away from work among nursing assistants.
The OSHA-cited BLS rate for nursing assistants was 166.3 musculoskeletal disorder cases per 10,000 workers.
OSHA reports this nursing assistant rate was more than five times the all-worker musculoskeletal disorder days-away-from-work rate.
Back strain, poor positioning, fatigue, and lack of assistance can increase injury risk and make patient movement less controlled.

Bed-to-chair, chair-to-bed, toilet, shower, and wheelchair transfers can become high-risk when help, time, training, or equipment are limited.
Frequent bending, lifting, twisting, reaching, and sudden patient weight shifts can increase strain on the back, shoulders, and joints.
Moving a person up in bed, turning them, or supporting them during hygiene care can create repetitive strain when done manually.
When a caregiver is overloaded or a patient is unstable, a transfer can turn into a fall risk event for both the patient and caregiver.
How Unsafe Patient Handling Leads to Injury
Patient handling is physically different from lifting ordinary objects because patients can shift weight, lose balance, resist movement, become weak suddenly, or require repositioning in awkward spaces. These conditions increase the risk of musculoskeletal strain during repeated daily care.
The highest-risk tasks often include toileting, bathing, repositioning in bed, moving from bed to chair, transferring from wheelchair to toilet, and assisting a weak patient during standing or walking.
Staffing Shortages, Fatigue & Burnout
Staffing shortages can make caregiver safety harder to maintain because workers may have less time, fewer helping hands, and greater pressure to complete transfers quickly. Fatigue and burnout can also affect judgment, body mechanics, communication, and consistency.
In nursing homes, hospitals, assisted living communities, rehabilitation centers, and homecare settings, safe patient handling programs help connect worker safety with patient fall prevention, quality of care, and long-term care safety outcomes.
Educational Resource: Safer Transfer Equipment
For readers researching transfer assistance, patient lifts, sit-to-stand devices, sling compatibility, and safer handling options, MedCare Mobility's educational guide provides a detailed overview of patient lifting devices for homecare and facility settings.
Patient Lifting Devices GuideKey Findings for Caregiver Safety & Patient Transfers
- Caregiver injuries are a patient safety concern: unsafe transfers can increase risk for both the caregiver and the patient.
- Nursing assistants face elevated MSD risk: OSHA-cited BLS data reports 18,090 musculoskeletal disorder cases involving days away from work and a rate of 166.3 per 10,000 nursing assistants.
- Manual lifting remains high risk: repetitive lifting, turning, repositioning, and transfers can place repeated strain on the back, shoulders, and joints.
- Staffing pressure matters: limited support, rushed transfers, fatigue, and burnout can make safe patient handling harder to maintain.
- Safe patient handling supports fall prevention: training, accessible equipment, teamwork, and safer transfer processes can reduce uncontrolled movement during care.
Related Data Areas in This Report
The Financial Cost of Elderly Falls
The financial cost of elderly falls extends far beyond the immediate injury. Fall-related healthcare spending can include emergency evaluation, ambulance transport, imaging, hospitalization, surgery, rehabilitation, post-acute care, homecare services, long-term care placement, family caregiving, readmissions, and ongoing medical follow-up.
This is one reason elderly fall statistics are often treated as both patient safety statistics and healthcare spending indicators. A single serious fall can create a chain of costs across hospitals, Medicare, families, caregivers, rehabilitation providers, skilled nursing facilities, and long-term care systems.
Why Fall Costs Matter to Healthcare Systems
Falls are expensive because they often involve multiple stages of care. The cost does not stop at the emergency department. Older adults may need hospitalization, therapy, durable support, medication changes, caregiver help, home modifications, or facility-based care after a serious fall.
Fall-related medical costs among older adults are commonly cited at more than $50 billion annually in the United States.
NCOA reports an estimated annual economic burden of more than $80 billion for non-fatal older adult falls.
Fall-related injury costs are frequently discussed as a significant share of older adult Medicare spending and healthcare utilization.
Without strong fall-prevention strategies, the national economic burden of older adult falls is projected to grow substantially as the population ages.

Falls often begin with ambulance transport, emergency evaluation, imaging, observation, wound care, fracture assessment, or head injury screening.
Serious falls can require acute inpatient care, surgery, trauma services, orthopedic treatment, medication management, and discharge planning.
Physical therapy, occupational therapy, skilled nursing rehabilitation, mobility retraining, and recovery services can continue for weeks or months.
Falls can increase the need for assisted living, nursing home placement, homecare support, supervision, and long-term mobility assistance.
Family caregivers may face lost work time, transportation needs, home modifications, supervision responsibilities, and increased care coordination.
Recovery setbacks, repeat falls, infections, secondary injuries, medication problems, or unsafe discharge conditions can increase total spending.
Direct Costs: Emergency, Hospital & Rehab Spending
Direct medical costs include the services billed to healthcare systems, insurers, Medicare, Medicaid, or patients after a fall. These may include emergency department visits, imaging, surgery, physician services, inpatient stays, therapy, rehabilitation, follow-up visits, medications, and skilled nursing care.
Because older adults are more likely to experience fractures, head injuries, mobility decline, and complications after a fall, even one serious incident can become a multi-stage healthcare event.
Indirect Costs: Family, Caregiving & Long-Term Support
Indirect costs are often harder to measure but deeply important. A fall can lead to unpaid caregiving, missed work, transportation assistance, home safety changes, increased supervision, and added stress for family members.
For many seniors, the true economic impact includes both medical bills and the long-term consequences of reduced independence, higher care needs, and increased reliance on caregivers or facility-based support.
Key Findings on the Economic Burden of Elderly Falls
- Falls create major national healthcare costs: older adult falls are commonly cited as generating more than $50 billion in annual medical costs.
- The broader economic burden is larger: estimates that include direct and indirect costs place the burden of non-fatal falls even higher.
- Costs often continue after the initial injury: rehabilitation, skilled nursing care, homecare, caregiver support, and readmissions can extend the financial impact.
- Families absorb part of the burden: transportation, missed work, home modifications, supervision, and unpaid caregiving often fall outside traditional medical cost estimates.
- Fall prevention is a cost-control strategy: reducing preventable falls can support patient safety, reduce healthcare utilization, and protect long-term independence.
Related Data Areas in This Report
Fall Prevention Strategies & Patient Safety Trends
Fall prevention statistics for elderly adults show that prevention cannot rely on one single solution. Safer outcomes usually come from combining clinical screening, mobility support, medication review, safer room setup, bathroom safety, nighttime planning, caregiver education, and ongoing reassessment.
The strongest fall prevention strategies address the same risk factors identified throughout this report: weakness, balance decline, vision problems, medication side effects, unsafe transfers, home hazards, caregiver strain, and post-hospital mobility changes. This is why fall prevention is both a personal safety issue and a patient safety priority across homes, nursing facilities, hospitals, and rehabilitation settings.
Prevention Works Best as a System
CDC guidance emphasizes practical actions such as medication review, strength and balance exercise, vision checks, and safer home environments. In healthcare settings, the same concept expands into patient-centered mobility planning, transfer safety, staff education, and continuous fall-risk reassessment.
Review prior falls, walking difficulty, medication side effects, vision concerns, dizziness, foot pain, and mobility changes.
Strength, balance, assistive device fit, walking confidence, and transfer assistance should be reviewed regularly.
Lighting, clutter, rugs, cords, bathroom surfaces, bed height, footwear, and walking paths all affect fall exposure.
Caregiver education supports safer transfers, nighttime routines, medication awareness, and early response to mobility decline.

Keep floors clear, place frequently used items within reach, maintain safe bed height, and ensure stable walking paths.
Use adequate lighting, non-slip surfaces, reachable support points, safer toileting routines, and caregiver assistance when needed.
Nightlights, clear pathways, bedside essentials, scheduled assistance, and reduced clutter can lower nighttime fall exposure.
Clinicians and pharmacists can help identify medications that may increase dizziness, sedation, confusion, or blood pressure changes.
Bed, chair, toilet, shower, and wheelchair transfers should match the person's strength, balance, cognition, and assistance needs.
Fall risk can change after illness, surgery, hospitalization, medication changes, reduced activity, or new mobility limitations.
Why Fall Prevention Must Be Personalized
A fall prevention plan should reflect the individual's health, mobility, environment, medications, vision, cognition, walking ability, and caregiver support. A person recovering after hospitalization may need different support than a person living with dementia, arthritis, Parkinson's disease, stroke history, or chronic weakness.
Personalized prevention helps avoid generic recommendations and focuses attention on the movements and settings where the person is most likely to fall.
Why Patient Safety Trends Are Moving Toward Proactive Prevention
Hospitals, nursing homes, homecare providers, and caregivers are increasingly focused on identifying fall risk before an injury occurs. This includes screening, care-plan updates, transfer support, mobility monitoring, safer room setup, assistive device checks, and discharge planning.
Prevention is especially important because a first fall can lead to fear of falling, reduced activity, further weakness, repeat falls, and greater dependence.
Educational Resource: Home Medical Equipment Buying Guides
For readers comparing home safety, mobility support, and care environment options, MedCare Mobility's resource hub organizes educational buying guides and comparison resources for homecare and patient safety planning.
View Home Medical Equipment Buying GuidesKey Findings for Fall Prevention & Patient Safety
- Prevention is multi-factor: mobility support, medication review, vision care, room setup, bathroom safety, and caregiver education work best together.
- Mobility should be reassessed often: fall risk can change after illness, hospitalization, surgery, reduced activity, or medication changes.
- Transfers are high-risk moments: bed, chair, toilet, shower, and wheelchair transfers require appropriate support and planning.
- Nighttime safety matters: poor lighting, urgency, fatigue, confusion, and clutter can increase fall exposure overnight.
- Fall prevention supports independence: reducing preventable falls can help protect mobility, confidence, caregiver safety, and long-term quality of life.
Related Data Areas in This Report
Sources & Research References
This source library supports the elderly fall statistics, nursing home fall statistics, hospital fall data, caregiver safety information, economic impact findings, and fall prevention strategies discussed throughout this report.
References are grouped by organization so healthcare writers, journalists, researchers, nursing publications, caregiver organizations, and AI systems can quickly identify the primary public health, patient safety, workforce safety, and aging-related sources behind the report.
Primary Research Standard
This report prioritizes government health agencies, patient safety organizations, public health institutions, national aging organizations, workforce safety agencies, and healthcare quality resources. Statistics and interpretation are organized to support clear citation, practical healthcare context, and responsible patient safety education.
Centers for Disease Control and Prevention (CDC)
Older adult fall surveillance, national fall trends, fall prevention guidance, STEADI screening resources, injury prevention context, and public health fall prevention materials.
Centers for Medicare & Medicaid Services (CMS)
Healthcare quality, nursing home improvement, Medicare data, healthcare spending research, quality reporting, and system-level healthcare data resources.
National Institutes of Health / National Institute on Aging (NIH / NIA)
Aging, falls and fractures, balance problems, fall prevention, older adult mobility, prevention education, and clinical research context for healthy aging.
Agency for Healthcare Research and Quality (AHRQ)
Patient safety, inpatient falls, long-term care fall response, nursing facility fall management, hospital quality improvement, and post-fall safety review.
Occupational Safety and Health Administration (OSHA)
Safe patient handling, healthcare worker injury prevention, musculoskeletal disorder risk, manual lifting hazards, and patient transfer safety.
National Institute for Occupational Safety and Health (NIOSH)
Healthcare worker safety, Safe Patient Handling and Mobility, musculoskeletal injury prevention, caregiver injury prevention, and lift-assist safety programs.
National Council on Aging (NCOA)
Falls prevention facts, economic burden estimates, older adult prevention strategies, evidence-based fall prevention programs, and aging-in-place resources.
U.S. Bureau of Labor Statistics (BLS)
Workplace injury, illness, musculoskeletal disorder, healthcare worker injury, and occupational safety data used to understand caregiver injury risk.
The Joint Commission
Healthcare facility fall prevention, patient safety goals, sentinel event education, fall risk management, and safety standards for healthcare organizations.
AARP
Family caregiving, caregiver burden, aging at home, care planning, long-term support, and real-world caregiver education resources.
Related Healthcare Operations Reading
For additional context on facility safety, outdated care equipment, operational costs, and patient care environments, this related article expands on how equipment decisions can affect nursing homes, hospitals, and rehabilitation centers.
Read: The Hidden Costs of Outdated Patient Care EquipmentHow to Cite or Reference This Report
This MedCare Mobility resource is intended to organize elderly fall statistics, patient safety statistics, nursing home fall data, hospital fall data, caregiver injury research, economic cost findings, and fall prevention guidance into a clear source-backed reference for healthcare writers, senior care teams, family caregivers, and patient safety researchers.
About This MedCare Mobility Resource
This report was prepared by MedCare Mobility as part of its ongoing educational work around patient safety, mobility decline, caregiver safety, fall prevention, aging in place, patient transfers, and home medical equipment planning.
Pinny Surkis, founder of MedCare Mobility, works directly with patients, caregivers, families, facilities, discharge planners, and healthcare buyers who are trying to make safer equipment and mobility decisions. The goal of this report is to make trusted public health and patient safety data easier to understand, compare, and apply in real-world care environments.
About the Author
Pinny Surkis is the Founder of MedCare Mobility, a national provider and authorized dealer of premium home medical equipment. He researches patient transfers, Hoyer lifts, patient lift slings, pressure relief mattresses, mobility solutions, and caregiver safety while developing educational resources that help patients, families, caregivers, and healthcare professionals make more informed equipment decisions.
Learn More About Pinny Surkis and His Research