


16
Jun
Bed Sores & Pressure Ulcers: Prevention, Early Warning Signs, Stages, Risk Factors, Pressure Relief & Patient Safety Guide
Start With Prevention
Bed Sore Prevention Starts Before Skin Breaks Down
A small red area on the tailbone, heel, hip, or buttocks can seem minor at first. But for bedridden patients, wheelchair users, elderly adults, and nursing home residents, early skin changes can be the first warning sign of pressure-related tissue damage.
Maybe you noticed a sore heel after several days in bed. Maybe a parent says their buttocks hurt after sitting in a wheelchair. Maybe you are worried about skin breakdown in a nursing home, assisted living facility, rehab center, or home care setting. This guide is designed to help caregivers understand what bed sores are, why pressure ulcers happen, what early warning signs to watch for, and how daily prevention routines can reduce risk.
The terms bed sores, pressure ulcers, pressure injuries, and skin breakdown are often used together. In everyday caregiving, many people still say “bed sores.” In clinical education, the more current term is often pressure injury because tissue damage may begin before the skin fully opens.
Bed Sores
The common caregiver term for pressure-related skin damage, especially in patients who spend long periods in bed.
Pressure Ulcers
A widely used medical term for wounds caused by pressure, often over bony areas like the tailbone, hips, or heels.
Pressure Injuries
The more current clinical term, because pressure damage can exist as intact skin or an open wound.
Skin Breakdown
A general phrase caregivers may use when skin becomes irritated, weakened, discolored, blistered, or open.
The National Pressure Injury Advisory Panel defines a pressure injury as localized damage to the skin and underlying soft tissue, usually over a bony prominence or related to a medical device, caused by pressure or pressure combined with shear. AHRQ reports that pressure ulcers affect more than 2.5 million people in the United States each year and are associated with pain, infection risk, and increased healthcare use.
Who This Guide Helps
- Family caregivers caring for an elderly parent at home
- Home health aides and private-duty caregivers
- Wheelchair users concerned about sitting pressure
- Bedridden patients and people with limited mobility
- Nursing assistants, nurses, and daily care teams
- Assisted living and nursing home staff
- Hospital discharge planners and rehab facilities
- Long-term care administrators building prevention routines
What This Guide Covers
- Why bed sores happen and how pressure reduces blood flow
- Where pressure ulcers commonly develop on the body
- Early warning signs caregivers should not ignore
- Who is most at risk for pressure injuries
- Pressure ulcer stages and what they generally mean
- Daily pressure ulcer prevention strategies
- Pressure relief mattresses and wheelchair cushions
- Nursing home, assisted living, hospital, and rehab prevention practices
To prevent bed sores, it helps to first understand where pressure injuries form and what caregivers should watch for early.
Why Sores Form
Why Bed Sores Happen: Pressure, Friction, Shear, Moisture & Reduced Blood Flow
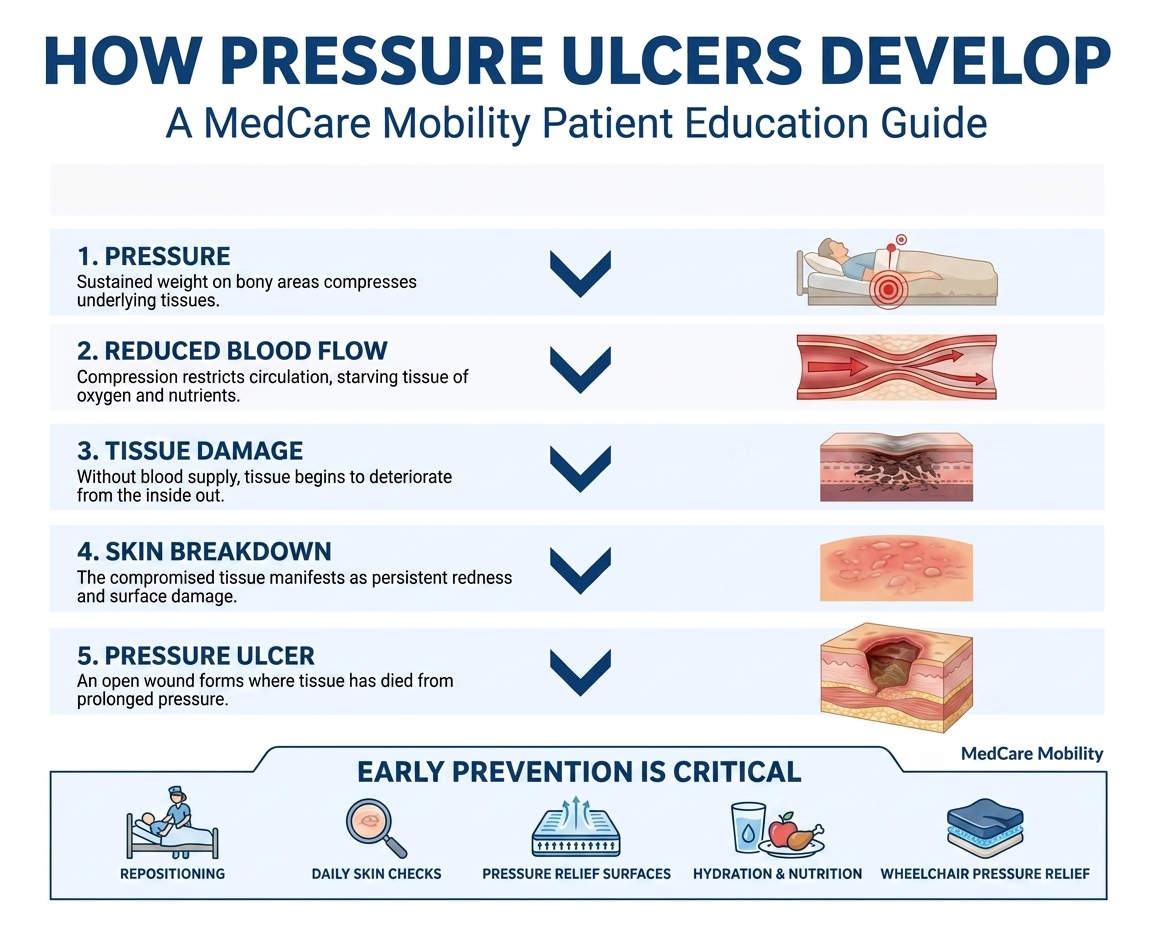
Bed sores are not just ordinary skin irritation. They usually begin when pressure, friction, shear, moisture, or reduced blood flow places stress on the skin and deeper tissue. For a bedridden patient, wheelchair user, elderly adult, or anyone with limited mobility, prevention needs to start before the skin opens.
1. Pressure
Pressure happens when body weight presses skin and tissue between a bony area and a surface, such as a mattress, wheelchair seat, recliner, hospital bed, or chair. The highest-risk areas are often the tailbone, buttocks, hips, heels, elbows, and shoulders.
2. Reduced Blood Flow
When pressure lasts too long, it can compress small blood vessels. Less blood flow means less oxygen and fewer nutrients reach the tissue. If pressure is not relieved, tissue damage can begin under the skin before a wound is visible.
3. Shear
Shear happens when the skin stays in place while deeper tissue moves. A common example is when a patient slides down in bed while the skin drags against the sheets. This is especially important with hospital beds, adjustable beds, and elevated head positions.
4. Friction
Friction occurs when skin rubs against bedding, clothing, wheelchair fabric, or transfer surfaces. It can weaken the outer layer of skin, making it easier for pressure ulcers and skin breakdown to develop.
5. Moisture
Sweat, urine, stool, wound drainage, or damp bedding can soften the skin. Moist skin is more fragile, more likely to tear, and more vulnerable to pressure-related damage, especially when moisture combines with friction or shear.
What This Means in Real Care
A pressure sore can form from long hours in bed, prolonged sitting in a wheelchair, sliding down in an elevated hospital bed, damp bedding, difficult transfers, or repeated rubbing against a surface. That is why pressure ulcer prevention has to address the full care environment — not just the skin spot that becomes visible later.
Why This Matters
Many pressure injuries begin before the skin visibly opens. By the time an open wound appears, tissue damage may already be developing beneath the surface.
What Caregivers Should Remember
A pressure ulcer prevention plan is not only about avoiding wounds. It is about reducing the conditions that allow pressure, moisture, friction, and shear to build up in the first place.
| Cause | What It Means | Common Example |
|---|---|---|
| Pressure | Body weight compresses tissue | Lying on the tailbone or heels |
| Shear | Skin and tissue move in opposite directions | Sliding down in bed |
| Friction | Skin rubs against a surface | Transfers or repositioning |
| Moisture | Skin becomes damp and fragile | Incontinence or sweating |
| Reduced blood flow | Tissue receives less oxygen | Prolonged sitting or lying |
Pressure
MeaningBody weight compresses tissue
ExampleLying on the tailbone or heels
Shear
MeaningSkin and tissue move in opposite directions
ExampleSliding down in bed
Friction
MeaningSkin rubs against a surface
ExampleTransfers or repositioning
Moisture
MeaningSkin becomes damp and fragile
ExampleIncontinence or sweating
Reduced Blood Flow
MeaningTissue receives less oxygen
ExampleProlonged sitting or lying
Once you understand how pressure injuries form, the next step is knowing what to watch for and who needs the most prevention support.
Common Pressure Points
Where Pressure Ulcers Commonly Develop: Tailbone, Buttocks, Heels, Hips & Other Pressure Points
Pressure ulcers usually form over bony areas where there is less natural padding between the skin and bone. That is why caregivers often first notice a sore on the tailbone, a pressure sore on the buttocks, a heel sore from bed rest, or skin breakdown around the hip, ankle, elbow, or shoulder.
Lying on Back
When a patient lies on their back for long periods, pressure can concentrate along the back of the body.
- Back of head
- Shoulder blades
- Elbows
- Sacrum / tailbone
- Buttocks
- Heels
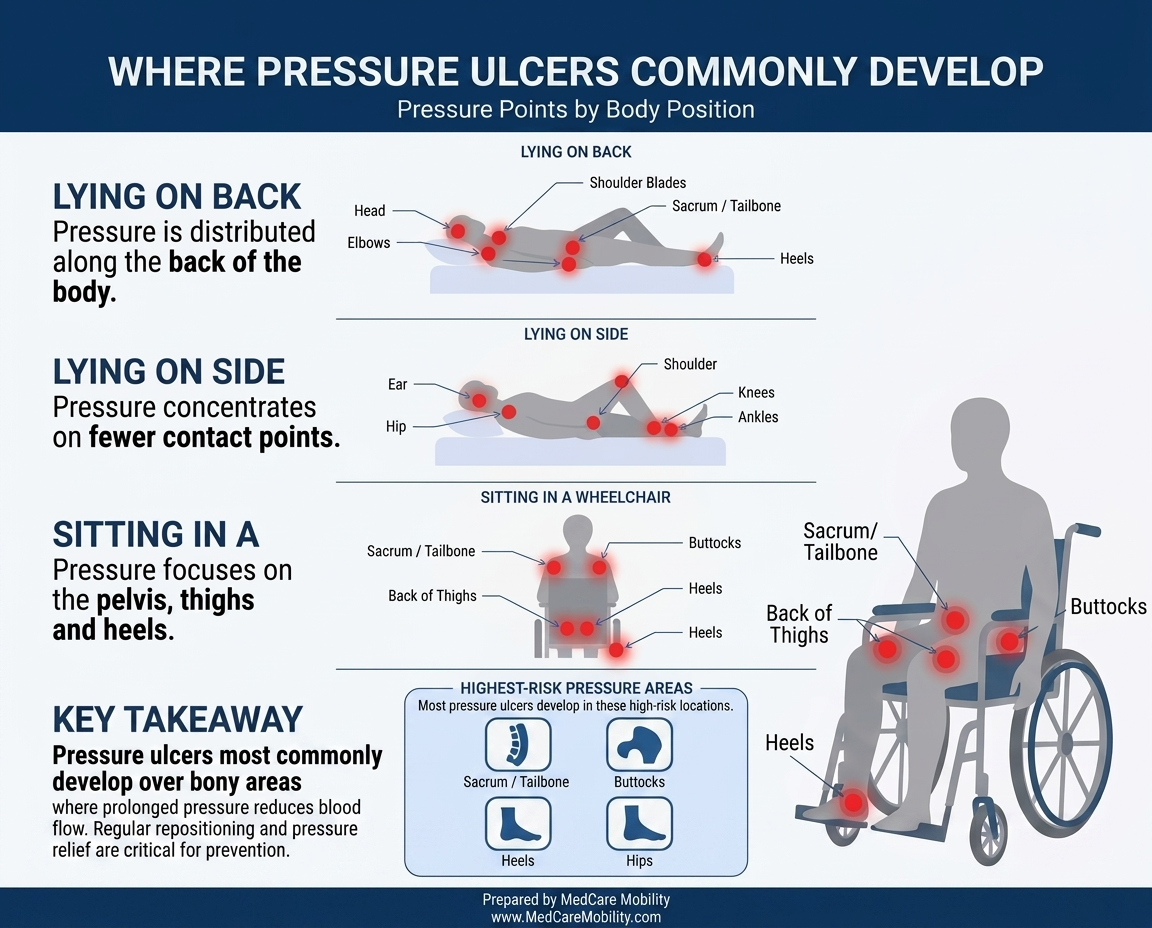
Lying on Side
Side-lying can create focused pressure on narrower bony areas, especially when the patient cannot shift position independently.
- Ear
- Shoulder
- Hip
- Knees
- Ankles
Sitting in Wheelchair
Wheelchair pressure sores often develop because prolonged sitting concentrates pressure on the pelvis and seating surface.
- Sacrum / tailbone
- Buttocks
- Back of thighs
- Heels if poorly positioned
- Shoulder blades if posture is poor
The Three Highest-Risk Areas to Watch Closely
| Patient Position | Common Pressure Points | Why It Matters |
|---|---|---|
| Lying on back | Sacrum, heels, elbows, shoulder blades | Long periods in bed can concentrate pressure on the back of the body |
| Lying on side | Hip, shoulder, ankle, knee, ear | Side-lying can create focused pressure on narrow bony areas |
| Sitting in wheelchair | Buttocks, sacrum, thighs, heels | Prolonged sitting increases pressure on the pelvis and seating surface |
Lying on Back
PointsSacrum, heels, elbows, shoulder blades
WhyLong periods in bed can concentrate pressure on the back of the body
Lying on Side
PointsHip, shoulder, ankle, knee, ear
WhySide-lying can create focused pressure on narrow bony areas
Sitting in Wheelchair
PointsButtocks, sacrum, thighs, heels
WhyProlonged sitting increases pressure on the pelvis and seating surface
Pressure points show where skin breakdown often begins. The next step is recognizing warning signs early and matching prevention to the patient’s risk level.
Early Warning Signs
Early Warning Signs of Bed Sores and Pressure Ulcers
Many caregivers first search because they noticed something specific: a red area on the tailbone, heel redness after bed rest, skin discoloration from sitting, or a sore spot on the buttocks of an elderly parent. The most important question is simple: is this red spot serious?
Do Not Wait for an Open Wound
Early bed sore symptoms can be subtle. A pressure injury may begin as redness that does not fade, darker discoloration, warmth, tenderness, swelling, burning, or a change in skin texture. For bedridden patients and wheelchair users, these early signs deserve attention before skin breakdown becomes more serious.
What Caregivers Are Usually Seeing
A Stage 1 pressure ulcer may still have intact skin. That means the area may not look like a wound yet, but the tissue may already be irritated from pressure, friction, shear, or reduced blood flow.
Color Changes
Redness, darker discoloration, purple areas, brownish changes, blue-gray tones, or ashen skin can all be early pressure ulcer symptoms.
Temperature Changes
The skin may feel warmer than nearby areas, especially around the tailbone, buttocks, heels, hips, ankles, elbows, or shoulders.
Pain or Burning
A patient may report tenderness, pain, burning, soreness, or discomfort when sitting, lying, repositioning, or transferring.
Texture Changes
The area may feel firm, hard, soft, boggy, shiny, swollen, or different from the skin around it.
Blisters or Open Skin
A blister, shallow opening, scrape-like area, or broken skin may suggest that pressure-related skin damage has progressed.
Drainage or Odor
Fluid, drainage, odor, blackened tissue, fever, or increasing pain may suggest infection concern and should be medically evaluated.
Pressure Injuries Can Look Different on Different Skin Tones
Do not rely only on the word “redness.” On darker skin tones, an early pressure injury may appear darker purple, blue-gray, brownish, ashen, shiny, warmer, firmer, or more painful than the surrounding skin.
Daily Skin Check Areas
- Tailbone / sacrum
- Buttocks
- Heels
- Hips
- Ankles
- Elbows
- Shoulders
- Back of head
- Areas under medical devices
- Areas under braces, cushions, or straps
Seek Medical Evaluation If You Notice:
- Redness or discoloration that does not fade
- Open skin
- Blisters
- Drainage
- Odor
- Increasing pain
- Warmth or swelling
- Blackened tissue
- Fever or signs of infection
Free Download: Bed Sore Prevention Checklist
Use this printable checklist to help track daily skin checks, repositioning, moisture control, nutrition, mobility, and pressure relief routines.
Healthy People notes that finding and treating pressure ulcers early is key to preventing related hospitalizations among older adults.
| Warning Sign | What It May Suggest | What to Do |
|---|---|---|
| Redness or discoloration | Early pressure injury risk | Relieve pressure and monitor closely |
| Warmth or swelling | Tissue irritation or inflammation | Notify caregiver or clinician |
| Blister | Skin damage | Avoid pressure and seek advice |
| Open wound | Possible advanced injury | Seek medical evaluation |
| Drainage or odor | Possible infection concern | Seek medical care promptly |
Redness or Discoloration
May suggestEarly pressure injury risk
What to doRelieve pressure and monitor closely
Warmth or Swelling
May suggestTissue irritation or inflammation
What to doNotify caregiver or clinician
Blister
May suggestSkin damage
What to doAvoid pressure and seek advice
Open Wound
May suggestPossible advanced injury
What to doSeek medical evaluation
Drainage or Odor
May suggestPossible infection concern
What to doSeek medical care promptly
Early warning signs matter most when a patient already has a higher risk of skin breakdown or limited ability to reposition independently.
High-Risk Patients
Who Is Most at Risk for Bed Sores and Pressure Injuries?
Bed sores can affect many types of patients, not only older adults in nursing homes. The risk increases when a person has limited mobility, reduced sensation, poor circulation, moisture exposure, difficulty repositioning, or a condition that makes skin more fragile.
Risk Usually Starts With One Simple Problem: The Patient Cannot Relieve Pressure Easily
A patient may not be able to turn in bed, shift weight in a wheelchair, feel early discomfort, stay dry, or ask for help quickly enough. That is why pressure ulcer prevention needs to match the patient’s real daily care situation.
Caregiver Question to Ask
“Can this patient move, feel pressure, stay dry, and reposition without help?” If the answer is no, the patient may need a more consistent bed sore prevention routine.
Bedridden Patients
Long periods in bed, less movement, and difficulty changing position can increase pressure on the heels, sacrum, hips, shoulders, and elbows.
Wheelchair Users
Wheelchair pressure sore risk increases with long sitting, especially on the buttocks, thighs, sacrum, and tailbone. Posture and cushion quality matter.
Stroke Recovery Patients
Weakness on one side, reduced sensation, and less ability to reposition can make stroke patients more vulnerable to bed sores and skin breakdown.
Spinal Cord Injury or Paralysis
Reduced sensation and limited movement may prevent a patient from feeling pain, pressure, or early warning signs before tissue damage progresses.
Diabetes or Poor Circulation
Diabetes pressure ulcer risk can increase because of reduced sensation, slower healing, circulation problems, and greater foot or heel concern.
Incontinence
Moisture from urine, stool, sweating, or damp bedding can weaken skin and increase the risk of pressure injuries, especially when combined with friction.
Malnutrition or Dehydration
Skin needs nutrition, protein, and hydration to stay resilient. Poor appetite, weight loss, or dehydration can make skin more vulnerable.
Advanced Age
Elderly skin breakdown risk increases when skin becomes thinner, natural padding decreases, mobility declines, and recovery takes longer.
Bariatric Patients
Bariatric patient pressure injury risk can increase because of higher pressure loads, moisture and skin-fold challenges, and more difficult transfers or repositioning.
Three Risk Patterns Caregivers Should Notice
Less movement: the patient cannot shift, turn, stand, or reposition without help.
Less sensation: the patient may not feel pain, pressure, burning, or discomfort early.
More moisture or friction: the skin is exposed to dampness, rubbing, sliding, or difficult transfers.
Less skin resilience: poor circulation, poor nutrition, diabetes, age, or illness makes skin more fragile.
High-Risk Patients Need Prevention Before Skin Breaks Down
If a patient cannot easily move, feel discomfort, stay dry, or reposition independently, pressure injury prevention should become part of daily care.
Support Surface Questions
For families comparing support surfaces, our hospital bed mattress questions page explains common mattress terms in plain language.
| Risk Level | Patient Profile | Prevention Priority |
|---|---|---|
| Lower Risk | Mobile, good nutrition, no skin changes | Routine skin checks and activity |
| Moderate Risk | Limited mobility, wheelchair use, occasional incontinence | Repositioning schedule, cushion/mattress review |
| High Risk | Bedridden, poor circulation, diabetes, prior pressure ulcer, incontinence | Daily skin checks, pressure relief surfaces, care plan review |
| Very High Risk | Open wound, repeated ulcers, severe immobility, facility-level care needs | Medical/wound care oversight and advanced prevention plan |
Lower Risk
ProfileMobile, good nutrition, no skin changes
PriorityRoutine skin checks and activity
Moderate Risk
ProfileLimited mobility, wheelchair use, occasional incontinence
PriorityRepositioning schedule, cushion/mattress review
High Risk
ProfileBedridden, poor circulation, diabetes, prior pressure ulcer, incontinence
PriorityDaily skin checks, pressure relief surfaces, care plan review
Very High Risk
ProfileOpen wound, repeated ulcers, severe immobility, facility-level care needs
PriorityMedical/wound care oversight and advanced prevention plan
Risk level helps caregivers decide how consistent prevention needs to be. The next step is turning that risk awareness into daily pressure ulcer prevention routines.
Pressure Ulcer Stages
Pressure Ulcer Stages Explained: Stage 1, Stage 2, Stage 3, Stage 4, Deep Tissue Injury & Unstageable Wounds
Pressure ulcer stages help describe how deep or serious a pressure injury may be. This section is educational and should not replace diagnosis, wound staging, or treatment guidance from a qualified healthcare professional.
Why Staging Matters
Many people search “what does a Stage 1 bedsore look like?” because the skin may still be intact. Understanding the difference between Stage 1, Stage 2, Stage 3, Stage 4, deep tissue pressure injury, and unstageable wounds helps caregivers recognize why early action matters.
Staging Should Be Confirmed Clinically
Caregivers can watch for warning signs, but pressure injury staging should be confirmed by a qualified healthcare professional. Some wounds are deeper than they appear, and deep tissue injuries may begin below the skin surface.
Pressure Injury Stage Snapshot
Intact Skin
Red or discolored area, warmth, pain, firmness, softness, or skin that does not fade as expected.
Surface Damage
Partial-thickness skin loss that may look like a shallow open sore or blister.
Deeper Wound
Full-thickness skin loss where deeper tissue damage is present and fat may be visible.
Serious Tissue Damage
Deep tissue damage where muscle, tendon, ligament, cartilage, or bone may be exposed.
Deep Tissue Injury
Damage may begin beneath intact skin and appear purple, maroon, darker, painful, firm, or boggy.
Depth Not Yet Clear
Wound depth cannot be confirmed because tissue, slough, or eschar covers the base.
Stage 1 Pressure Injury
- Skin is intact.
- The area may be red or discolored.
- It may feel warm, painful, firm, or soft.
- The color may not blanch or fade as expected when pressure is relieved.
Stage 2 Pressure Injury
- Partial-thickness skin loss is present.
- It may look like a shallow open sore or blister.
- The surface layer of skin is damaged.
- Caregivers should avoid continued pressure and seek clinical guidance.
Stage 3 Pressure Injury
- Full-thickness skin loss is present.
- Damage extends deeper into tissue.
- Fat may be visible.
- This requires medical care and wound care oversight.
Stage 4 Pressure Injury
- Deep tissue damage is present.
- Muscle, tendon, ligament, cartilage, or bone may be exposed.
- This is a serious medical concern.
- Prompt wound care evaluation is important.
Deep Tissue Pressure Injury
- Damage may begin beneath intact skin.
- The area may appear purple, maroon, darker, painful, firm, or boggy.
- The surface may not show the full extent of underlying tissue damage.
- This can be especially important when skin color changes are subtle.
Unstageable Pressure Injury
- The wound depth cannot be confirmed.
- Slough, eschar, or tissue may cover the wound base.
- Clinical evaluation is needed to understand the true depth.
- Caregivers should not attempt to stage these wounds themselves.
Early Does Not Mean Minor
A Stage 1 pressure injury may look small, but it can signal that tissue is already under stress. Early action can help prevent progression.
The National Pressure Injury Advisory Panel pressure injury staging system is widely used in U.S. pressure injury education and describes Stage 1, Stage 2, Stage 3, Stage 4, deep tissue pressure injury, and unstageable pressure injury.
| Stage | What It May Look Like | Skin Surface | Why It Matters |
|---|---|---|---|
| Stage 1 | Red or discolored area | Intact | Earliest visible warning sign |
| Stage 2 | Blister or shallow open area | Broken | Skin surface is damaged |
| Stage 3 | Deeper wound | Full-thickness loss | Tissue damage extends deeper |
| Stage 4 | Deep wound | Severe tissue loss | Serious medical concern |
| Deep Tissue Injury | Purple, maroon, or dark area | May be intact | Damage may be beneath skin |
| Unstageable | Covered wound base | Cannot see depth | Needs clinical assessment |
Stage 1
Looks likeRed or discolored area
SurfaceIntact
WhyEarliest visible warning sign
Stage 2
Looks likeBlister or shallow open area
SurfaceBroken
WhySkin surface is damaged
Stage 3
Looks likeDeeper wound
SurfaceFull-thickness loss
WhyTissue damage extends deeper
Stage 4
Looks likeDeep wound
SurfaceSevere tissue loss
WhySerious medical concern
Deep Tissue Injury
Looks likePurple, maroon, or dark area
SurfaceMay be intact
WhyDamage may be beneath skin
Unstageable
Looks likeCovered wound base
SurfaceCannot see depth
WhyNeeds clinical assessment
Understanding pressure ulcer stages explains why daily prevention and pressure relief routines matter before wounds progress.
Daily Prevention Steps
How to Help Prevent Bed Sores: Daily Pressure Ulcer Prevention Strategies
Pressure ulcer prevention works best when it becomes a daily routine. For bedridden patients, wheelchair users, elderly adults, and high-risk patients, the goal is to reduce pressure, protect the skin, manage moisture, support nutrition, and make movement or repositioning part of regular care.
Prevention Is a Daily Care System
No single action prevents every bed sore. The strongest prevention plan combines repositioning, skin checks, moisture control, nutrition, mobility, safe transfers, and pressure relief support based on the patient’s condition and care plan.
Caregiver Goal
Do not wait until a pressure sore opens. Watch high-risk areas, respond to early skin changes, and reduce prolonged pressure before tissue damage progresses.
1. Repositioning
Repositioning helps relieve pressure before tissue damage progresses. Bedridden patients usually need consistent position changes according to their care plan, while wheelchair users may need weight shifts, tilt, recline, standing breaks, or caregiver-assisted repositioning.
2. Daily Skin Checks
Look daily at high-risk pressure areas. Skin checks should be routine, not only when pain appears, because some patients may not feel discomfort due to neuropathy, stroke, spinal cord injury, or reduced sensation.
3. Moisture Management
Keep skin clean and dry. Address incontinence quickly, change damp bedding or clothing, and use barrier products if recommended by a clinician.
4. Nutrition & Hydration
Skin needs adequate nutrition to stay resilient. Hydration and protein intake matter, and weight loss or poor appetite should be discussed with healthcare providers.
5. Mobility & Transfers
Even small amounts of safe movement can reduce prolonged pressure. Safe transfers help reduce dragging, friction, and shear, while patient lifts or transfer aids may reduce caregiver strain and skin-damaging movement.
Examples of Pressure Relief Movements
Turning from back to side according to the care plan
Floating heels when appropriate and clinically recommended
Shifting weight while seated in a wheelchair
Adjusting wheelchair posture and seating position
Reducing sliding down in bed to limit shear
Using proper transfer technique to avoid dragging skin
Daily Bed Sore Prevention Checklist
- Check skin over high-risk pressure areas
- Reposition according to the patient’s care plan
- Keep skin clean and dry
- Reduce friction during transfers
- Check mattress and cushion condition
- Encourage safe mobility when possible
- Monitor food and fluid intake
- Report new redness, discoloration, pain, drainage, or odor
Prevention Works Best as a Routine
Pressure ulcer prevention is not one single product or one single action. It is a daily routine that combines repositioning, skin inspection, moisture control, nutrition, mobility, and pressure relief.
Download the Printable Bed Sore Prevention Checklist
Use this printable checklist to track daily skin checks, repositioning, moisture control, nutrition, mobility, mattress condition, cushion condition, and pressure relief routines.
Cleveland Clinic notes that a nutritious, high-protein diet can help prevent bedsores or support healing, and that people at risk should check skin regularly for signs of bedsores.
Daily prevention is the foundation. For higher-risk patients, the right pressure relief surfaces and wheelchair cushions can help support the care plan between repositioning routines.
Pressure Relief Solutions
Pressure Relief Surfaces: Mattresses, Wheelchair Cushions & Positioning Equipment
Pressure relief surfaces are not a replacement for care. They are tools that support a pressure ulcer prevention plan. The right mattress, wheelchair cushion, positioning aid, or transfer support depends on the patient’s mobility, skin condition, moisture risk, sitting time, bed time, and ability to reposition.
Choose Support Based on the Patient’s Risk
A pressure relief mattress may help a bedridden patient. A wheelchair pressure relief cushion may help someone who sits for long periods. Heel protection may help when redness develops around the heels. Transfer aids may help when dragging, friction, or shear is part of the problem.
Support Surfaces Fit Into the Care Plan
The most helpful approach is to match the patient’s situation with the care concern: bed rest, wheelchair sitting, heel pressure, moisture, sliding, difficult transfers, or facility-wide prevention.
Foam Pressure Redistribution Mattresses
Foam pressure redistribution mattresses may be appropriate for prevention-focused care, short-term immobility, general comfort, and patients who can still reposition with help.
These mattresses are designed to help spread pressure more evenly instead of concentrating force on the tailbone, hips, shoulders, or heels.
Alternating Pressure Mattresses
Alternating pressure systems periodically shift pressure across different areas of the body. They may be considered when a patient spends long hours in bed and has difficulty repositioning independently.
They are often discussed for elevated risk patients, prolonged bed rest, recurring pressure concerns, and dynamic pressure redistribution needs.
Low Air Loss Mattresses
Low air loss mattresses may be considered when moisture, heat, and skin microclimate are part of the care concern, especially for higher-risk skin breakdown or more advanced care environments.
These systems may support patients who need pressure redistribution along with moisture or heat management.
Wheelchair Pressure Relief: Foam, Gel, Air & Hybrid Cushions
Wheelchair users face a different pressure problem because prolonged sitting concentrates pressure on the buttocks, sacrum, tailbone, back of thighs, and sometimes the heels if foot positioning is poor. A pressure relief cushion helps support seated pressure redistribution, posture, comfort, and skin protection.
Buttocks and sacrum: prolonged sitting can concentrate pressure directly under the pelvis.
Tailbone pain: coccyx discomfort may signal the need to review posture, cushion fit, and sitting time.
Back of thighs: seat depth, cushion height, and posture can affect thigh pressure.
Heels and feet: poor positioning may increase pressure or rubbing around the lower legs and heels.
| Cushion Type | General Use Case | Notes |
|---|---|---|
| Foam | Basic support and comfort | May be appropriate for lower-risk users |
| Gel | Comfort and pressure distribution | Often used for seated pressure relief |
| Air | Adjustable pressure redistribution | May help higher-risk seating needs |
| Hybrid | Combines materials | Can balance stability, comfort, and pressure relief |
Foam
Use caseBasic support and comfort
NotesMay be appropriate for lower-risk users
Gel
Use caseComfort and pressure distribution
NotesOften used for seated pressure relief
Air
Use caseAdjustable pressure redistribution
NotesMay help higher-risk seating needs
Hybrid
Use caseCombines materials
NotesCan balance stability, comfort, and pressure relief
Positioning Aids, Heel Protection & Transfer Support
Pressure relief is not only about mattresses and cushions. For some patients, positioning and transfer support are just as important because pressure injuries can be made worse by sliding, dragging, moisture, and poor body alignment.
Pillows and wedgesMay help support body alignment and reduce direct pressure when used appropriately.
Heel protectionMay help reduce heel pressure risk when a patient spends long periods in bed.
Positioning supportsMay help limit sliding, poor posture, or pressure concentration.
Transfer aids and patient liftsMay reduce dragging, friction, shear, and caregiver strain during difficult transfers.
| Situation | Common Support Option | Natural Next Step |
|---|---|---|
| Bedridden patient | Pressure relief mattress | Compare mattress types |
| Wheelchair user | Pressure redistribution cushion | Review cushion options |
| Heel pressure risk | Heel protection / positioning | Ask care team about heel offloading |
| Sliding down in bed | Positioning support | Review bed positioning setup |
| Difficult transfers | Transfer aid or patient lift | Improve transfer safety |
| Facility-wide prevention | Mattress, cushion, skin check, repositioning protocol | Build prevention program |
Bedridden Patient
SupportPressure relief mattress
Next stepCompare mattress types
Wheelchair User
SupportPressure redistribution cushion
Next stepReview cushion options
Heel Pressure Risk
SupportHeel protection / positioning
Next stepAsk care team about heel offloading
Sliding Down in Bed
SupportPositioning support
Next stepReview bed positioning setup
Difficult Transfers
SupportTransfer aid or patient lift
Next stepImprove transfer safety
Facility-Wide Prevention
SupportMattress, cushion, skin check, repositioning protocol
Next stepBuild prevention program
Bedridden Patients
- Pressure redistribution mattresses
- Positioning wedges
- Adjustable bed positioning
- Repositioning plan
Wheelchair Users
- Pressure relief cushions
- Seating posture
- Weight shifts
- Cushion fit
Long-Term Care Facilities
- Alternating pressure systems
- Low air loss mattresses
- Facility-wide prevention protocols
- Documentation
Home Caregivers
- Skin inspection routines
- Transfer safety
- Repositioning support
- Mattress and cushion review
Important: Support Surfaces Do Not Replace Repositioning
Mattresses and wheelchair cushions can help redistribute pressure, but they do not replace regular repositioning, skin checks, moisture control, nutrition, and medical guidance.
Pressure relief equipment works best when it supports the daily care plan, not when it replaces caregiver attention or clinical guidance.
Examples of Pressure Relief Equipment by Care Need
After identifying the patient’s main pressure risk, families and care teams can compare support options more thoughtfully. These examples show how pressure relief mattresses, wheelchair cushions, and positioning-focused surfaces may fit different prevention needs without replacing a care plan.
Wheelchair Users: Seated Pressure Relief
Consider these when the main concern is sitting pressure, buttock discomfort, tailbone pressure, posture, or wheelchair cushion fit.

Comfort M2 Gel Cushion
For seated pressure relief, anti-thrust positioning, and skin-protection support.
View Cushion
Alternating Pressure Seat Cushion
For users who may need dynamic seated pressure redistribution.
View Cushion
Protekt Supreme Cushion
For basic wheelchair comfort, positioning support, and foam pressure distribution.
View Cushion
Acta-Embrace Cushion
For wheelchair positioning, comfort, and seated skin-protection support.
View CushionBedridden Patients: Mattress Support
Consider these when the main concern is long hours in bed, reduced repositioning ability, heel or sacral pressure, moisture risk, or recurring skin breakdown.

Protekt 300 Foam Mattress
For prevention-focused pressure redistribution and general hospital bed support.
View Mattress
Invacare microAIR MA600
For higher-risk care needs involving pressure redistribution and low air loss support.
View Mattress
Protekt Supreme Support
For alternating pressure support when dynamic pressure relief may be needed.
View Mattress
Protekt Aire 3000
For alternating pressure and low air loss support in higher-risk bed care settings.
View MattressFor More Advanced Positioning Needs
When a patient needs more complex pressure management, such as lateral rotation support, care teams may also review advanced systems like the Protekt Aire 7000 lateral rotation mattress. These decisions should be based on the patient’s risk level, skin condition, mobility, and clinical care plan.
Facility Prevention Programs
Pressure Ulcer Prevention in Nursing Homes, Assisted Living, Hospitals & Rehab Facilities
In nursing homes, assisted living communities, hospitals, and rehab facilities, pressure ulcer prevention is not only a bedside task. It is a facility-wide patient safety process built around skin assessment, risk screening, repositioning, staff training, documentation, support surfaces, wheelchair seating, and quality improvement.
Facility Prevention Requires a System
A strong pressure injury prevention program helps teams identify high-risk residents early, respond to skin changes quickly, document care consistently, and match mattresses, wheelchair cushions, positioning equipment, and transfer support to the patient’s actual risk level.
Who This Section Speaks To
This guidance is especially relevant for administrators, directors of nursing, wound care nurses, procurement teams, rehab centers, assisted living operators, hospital discharge planners, and long-term care teams responsible for pressure injury prevention protocols.
Skin Assessment Programs
Facilities need admission skin checks, routine skin inspections, high-risk resident monitoring, and clear documentation so new redness, discoloration, heel changes, buttock pressure, or sacral skin breakdown is not missed.
Risk Screening
Risk screening tools, such as the Braden Scale, may help teams identify residents who need more consistent prevention. The goal is not just scoring risk, but turning risk into a practical prevention plan.
Repositioning Protocols
Staff consistency matters. Missed repositioning can increase risk, and wheelchair residents need seated pressure relief plans too, including posture review, cushion fit, weight shifting, and sitting tolerance.
Staff Training
CNAs and caregivers are often the first people to see early skin changes. Training should cover pressure ulcer warning signs, moisture, friction, shear, heel risk, wheelchair pressure points, and reporting steps.
Support Surface Planning
Facilities may need different mattress types for different patient risk levels. Wheelchair cushions should not be ignored, and bariatric or high-risk residents may need specific support surfaces and transfer-support equipment.
Documentation & Quality Improvement
Documentation helps teams track skin status, repositioning, moisture care, nutrition concerns, support surface changes, family communication, and escalation when pressure injury risk increases.
Facility Pressure Injury Prevention Checklist
- Admission skin assessment
- Daily high-risk skin checks
- Repositioning documentation
- Moisture management plan
- Nutrition and hydration monitoring
- Wheelchair seating review
- Mattress/support surface review
- Staff training
- Clear escalation process
- Family communication when skin changes occur
Equipment Supports the Care Plan
For facilities, pressure ulcer prevention often requires a combination of staff protocols, documentation, repositioning practices, pressure redistribution mattresses, wheelchair cushions, and transfer-support equipment. The equipment supports the care plan — it does not replace the care plan.
Medical Bed Mattress Planning
Facilities may need foam redistribution, alternating pressure, low air loss, bariatric, and higher-risk support surface options depending on resident needs and care plans.
Medical bed mattress optionsWheelchair Seating Review
Wheelchair residents need seated pressure relief planning too. Cushion type, posture, fit, sitting time, foot positioning, and skin checks all matter.
Wheelchair seat cushion optionsAHRQ’s Preventing Pressure Ulcers in Hospitals toolkit is designed to help hospital staff implement prevention practices through an interdisciplinary approach. CMS also discusses nursing home quality measures related to pressure ulcers and notes prevention steps such as repositioning, nutrition, and soft padding to reduce pressure on the skin on its nursing home quality measures page.
Facility programs work best when prevention is consistent, documented, and supported by the right care routines and equipment choices.
Common Caregiver Questions
Frequently Asked Questions About Bed Sores, Pressure Ulcers and Pressure Injury Prevention
These questions are organized for caregivers: what bed sores are, what early signs look like, how pressure ulcer stages work, how to prevent skin breakdown, which mattresses and wheelchair cushions may help, and what facilities should do to reduce pressure injury risk.
Quick Caregiver Reminder
The most important takeaway is that pressure ulcer prevention works best when caregivers act early, check skin consistently, and match daily care routines with the patient’s actual risk level.
Basic Questions
What are bed sores?
Bed sores are areas of skin and tissue damage that develop when pressure stays on one area of the body for too long. They often form over bony areas such as the tailbone, buttocks, hips, heels, ankles, elbows, shoulders, or back of the head. Bed sores are common in people who spend long hours in bed, sit in a wheelchair for extended periods, or cannot reposition independently. They are also called pressure ulcers or pressure injuries.
Are bed sores the same as pressure ulcers?
Yes, many people use the terms bed sores and pressure ulcers to describe the same general problem: pressure-related skin and tissue damage. “Bed sore” is the everyday caregiver term, while “pressure ulcer” is a more clinical term. Today, many healthcare professionals use “pressure injury” because damage can begin under intact skin before an open wound appears. All three terms are commonly used when discussing prevention, early warning signs, stages, and pressure relief support.
What is a pressure injury?
A pressure injury is localized damage to the skin or deeper tissue caused by pressure, often combined with shear. It usually develops over a bony area or under a medical device, brace, cushion, strap, or support surface. The term “pressure injury” is important because the skin may still be closed in the earliest stage. A red, discolored, painful, warm, firm, or boggy area may already signal tissue stress even before the skin opens.
What causes bed sores?
Bed sores are mainly caused by prolonged pressure that reduces blood flow to the skin and tissue. They can also be worsened by shear, friction, moisture, poor nutrition, poor circulation, and limited mobility. For example, a patient sliding down in bed may experience shear, while a wheelchair user sitting for long periods may develop concentrated pressure on the buttocks or tailbone. Prevention focuses on relieving pressure before tissue damage progresses.
Can bed sores happen at home?
Yes. Bed sores can happen at home when a patient spends long hours in bed, sits in a wheelchair for extended periods, has incontinence, has trouble moving, or cannot communicate pain or discomfort. Family caregivers may first notice a red area on the tailbone, heel redness after bed rest, or skin discoloration on the buttocks. Home prevention depends on daily skin checks, repositioning, moisture control, nutrition, mobility support, and appropriate mattresses or cushions when needed.
Are bed sores common in nursing homes?
Bed sores can occur in nursing homes because many residents have limited mobility, advanced age, chronic illness, incontinence, poor nutrition, wheelchair use, or a history of pressure injuries. Good facilities use skin assessments, risk screening, repositioning plans, documentation, staff training, support surfaces, and wheelchair seating reviews to help reduce risk. Families should ask how the facility checks skin, tracks repositioning, handles moisture, and responds when redness or skin breakdown appears.
Can wheelchair users get pressure ulcers?
Yes. Wheelchair users can develop pressure ulcers because sitting concentrates pressure on the buttocks, sacrum, tailbone, and back of the thighs. Risk increases when a person sits for long periods, cannot shift weight, has poor posture, uses a worn or inappropriate cushion, or has reduced sensation. Wheelchair pressure relief usually includes skin checks, weight shifts, posture review, proper cushion fit, foot positioning, and sometimes a pressure redistribution cushion such as foam, gel, air, or hybrid seating.
Are pressure ulcers painful?
Pressure ulcers can be painful, but not every high-risk patient feels pain early. Some patients have reduced sensation from diabetes, neuropathy, stroke, spinal cord injury, paralysis, or general weakness. That means caregivers should not rely only on pain as a warning sign. Redness, discoloration, warmth, swelling, firmness, softness, bogginess, drainage, odor, or open skin may all be important signs even when the patient reports little or no pain.
Are bed sores dangerous?
Bed sores can become serious if they progress or become infected. Early pressure injuries may look small, but deeper tissue may already be under stress. Advanced pressure ulcers can involve deeper tissue damage, drainage, infection risk, pain, longer recovery time, and increased care needs. The safest approach is to treat early skin changes seriously, relieve pressure quickly, monitor the area closely, and seek medical evaluation for open wounds, drainage, odor, blackened tissue, fever, or worsening pain.
Can pressure ulcers become infected?
Yes. Pressure ulcers can become infected, especially when the skin opens or tissue damage deepens. Warning signs may include drainage, odor, warmth, swelling, increasing pain, redness or discoloration spreading around the area, blackened tissue, fever, or a general decline in the patient’s condition. Caregivers should not try to manage possible infection alone. Any concern about infection should be evaluated by a qualified healthcare professional or wound care provider.
Early Signs and Symptoms
What is the first sign of a bed sore?
The first sign of a bed sore is often a change in skin color or texture over a pressure point. On lighter skin, this may look red. On darker skin, it may appear purple, blue-gray, brownish, ashen, shiny, or warmer than surrounding skin. The area may feel painful, tender, firm, soft, swollen, or boggy. A key concern is discoloration that does not fade after pressure is relieved.
What does a Stage 1 pressure ulcer look like?
A Stage 1 pressure injury usually has intact skin, but the area shows signs of pressure damage. It may appear red, darker, purple, brownish, blue-gray, shiny, warm, painful, firm, soft, or different from nearby skin. The area may not blanch or fade as expected when pressure is removed. Stage 1 is important because it is the earliest visible warning sign and may improve if pressure is relieved quickly and the care plan is adjusted.
Is redness on the tailbone always a bed sore?
Redness on the tailbone is not always a bed sore, but it should be taken seriously in a bedridden patient, wheelchair user, elderly adult, or nursing home resident. The tailbone is a common pressure point because body weight can press skin and tissue against the mattress or chair. If the redness does not fade, feels warm, painful, firm, soft, swollen, or returns repeatedly, caregivers should relieve pressure and seek clinical guidance.
What does skin breakdown look like?
Skin breakdown may look like redness, discoloration, shiny skin, a blister, a shallow open area, peeling, drainage, or a wound. It may also feel warmer, tender, swollen, firm, or boggy. On darker skin tones, early breakdown may be less red and more purple, brown, gray, ashen, or darker than surrounding skin. Skin breakdown around the tailbone, buttocks, heels, hips, or under devices should be monitored closely.
Why is the skin warm or tender?
Warm or tender skin may suggest tissue irritation, inflammation, or early pressure-related damage. When pressure reduces blood flow or shear stresses deeper tissue, the area may feel different from nearby skin. Warmth and tenderness are especially important when they occur over the tailbone, buttocks, heels, hips, ankles, elbows, shoulders, or under a medical device. Caregivers should relieve pressure, monitor closely, and seek medical evaluation if symptoms persist or worsen.
What does a pressure sore on the heel look like?
A heel pressure sore may begin as redness, darker discoloration, warmth, tenderness, pain, swelling, a blister, or a soft or boggy area on the heel. In bedridden patients, heels are vulnerable because they can press directly into the mattress for long periods. Heel pressure concerns should be addressed early with skin checks, pressure relief, appropriate positioning, and clinical guidance, especially if there is open skin, drainage, odor, or blackened tissue.
What does a pressure sore on the buttocks look like?
A pressure sore on the buttocks may start as redness, dark discoloration, warmth, tenderness, burning, pain, swelling, firm tissue, soft tissue, blistering, or open skin. Wheelchair users and people who sit for long periods are at higher risk because pressure concentrates under the pelvis. Buttock pressure sores can also be worsened by moisture, incontinence, friction, and sliding. Caregivers should check skin daily and review cushion fit, posture, and sitting time.
Can pressure injuries look different on darker skin?
Yes. Pressure injuries may look different on darker skin, and early damage may not appear bright red. Caregivers should look for darker purple, blue-gray, brownish, ashen, shiny, warmer, firmer, softer, swollen, painful, or unusual-looking areas. Comparing the area with nearby skin can help. A change that does not fade after pressure relief, especially over a bony area or under a device, should be taken seriously.
When should a caregiver call a doctor?
A caregiver should call a doctor or qualified healthcare professional if redness or discoloration does not fade, skin opens, a blister appears, drainage or odor develops, pain increases, the area becomes warm or swollen, tissue looks blackened, or the patient has fever or signs of infection. Caregivers should also seek guidance if the patient has diabetes, poor circulation, paralysis, severe immobility, recurring ulcers, or a wound that seems to worsen quickly.
What signs suggest infection?
Possible infection signs include drainage, pus, odor, increasing pain, warmth, swelling, spreading redness or discoloration, fever, blackened tissue, or a sudden decline in the patient’s condition. A wound that becomes deeper, wetter, more painful, or foul-smelling should be evaluated promptly. Pressure ulcer infections can become serious, so caregivers should not try to treat suspected infection with home care alone. Medical or wound care guidance is important.
Pressure Ulcer Stages
What are the stages of pressure ulcers?
Pressure ulcer stages describe the visible depth and severity of a pressure injury. Stage 1 involves intact skin with discoloration or tissue stress. Stage 2 involves partial-thickness skin loss, often a blister or shallow open area. Stage 3 involves full-thickness skin loss and deeper tissue damage. Stage 4 involves severe tissue loss where muscle, tendon, ligament, cartilage, or bone may be exposed. Deep tissue injury and unstageable wounds also require clinical evaluation.
What is a Stage 1 pressure injury?
A Stage 1 pressure injury is the earliest visible stage. The skin is still intact, but the area may be red, discolored, darker, warm, painful, firm, soft, or different from surrounding skin. It may not blanch or fade as expected after pressure is relieved. Stage 1 should not be ignored because tissue may already be under stress. Early pressure relief, skin checks, and care plan adjustments may help prevent progression.
What is a Stage 2 pressure ulcer?
A Stage 2 pressure ulcer involves partial-thickness skin loss. It may look like a shallow open sore, a blister, or a broken skin surface. At this point, the outer layer of skin is damaged and the area needs protection from further pressure, friction, shear, and moisture. Caregivers should seek clinical guidance rather than trying to stage or treat the wound without professional input.
What is a Stage 3 pressure ulcer?
A Stage 3 pressure ulcer involves full-thickness skin loss, meaning the wound extends deeper into tissue. Fat may be visible, and the wound usually requires medical or wound care oversight. Stage 3 wounds are more serious than surface irritation and should not be managed casually. Prevention, pressure relief, moisture control, nutrition, support surfaces, and clinical treatment planning become especially important at this stage.
What is a Stage 4 pressure ulcer?
A Stage 4 pressure ulcer is a serious wound involving deep tissue damage. Muscle, tendon, ligament, cartilage, or bone may be exposed. This requires prompt medical and wound care evaluation. Caregivers should not attempt to manage Stage 4 wounds with basic home care. Treatment planning, infection monitoring, pressure relief, nutrition, moisture management, and appropriate support surfaces should be guided by qualified healthcare professionals.
What is a deep tissue pressure injury?
A deep tissue pressure injury is damage that may begin beneath intact skin. It can appear as a purple, maroon, dark, painful, firm, soft, warm, or boggy area. The surface may not show the full extent of deeper tissue injury, which is why these areas require careful attention. Deep tissue injuries are important because they can progress even when the skin does not initially look open or severe.
What does unstageable pressure ulcer mean?
Unstageable means the true depth of the pressure ulcer cannot be confirmed because the wound base is covered by tissue, slough, or eschar. Since the depth cannot be clearly seen, clinical evaluation is needed. Caregivers should not try to stage these wounds themselves or remove tissue without professional guidance. An unstageable pressure injury may be serious and should be assessed by a qualified healthcare or wound care provider.
Can a Stage 1 pressure ulcer heal?
A Stage 1 pressure injury may improve when pressure is relieved early and the care plan is adjusted. This may include repositioning, skin monitoring, moisture control, nutrition support, cushion or mattress review, and reducing friction or shear. However, improvement depends on the patient’s risk level, circulation, mobility, skin condition, and overall health. If discoloration persists, worsens, becomes painful, or progresses to broken skin, caregivers should seek medical guidance.
Can pressure ulcers get worse quickly?
Yes. Pressure ulcers can worsen quickly in high-risk patients, especially those who are bedridden, have diabetes, poor circulation, incontinence, malnutrition, reduced sensation, paralysis, severe weakness, or a history of prior pressure injuries. Damage may begin under the skin before an open wound appears. That is why early pressure relief, daily skin checks, moisture control, repositioning, and timely clinical evaluation are important.
Should caregivers try to stage wounds themselves?
Caregivers can learn the general meaning of pressure ulcer stages, but they should not rely on self-staging for diagnosis or treatment decisions. Wounds can be deeper than they appear, and some pressure injuries are difficult to classify without clinical assessment. Caregivers should use staging information to understand urgency, communicate clearly with healthcare providers, and know when to seek medical or wound care guidance.
Prevention
How do you help prevent bed sores?
Bed sore prevention usually requires a daily routine, not one single action. Caregivers should check high-risk skin areas, reposition according to the care plan, keep skin clean and dry, reduce friction during transfers, encourage safe movement when possible, monitor food and fluid intake, and review mattress or cushion support. Prevention should be tailored to the patient’s risk level, skin condition, mobility, and clinician recommendations.
How often should a bedridden patient be repositioned?
The exact repositioning schedule should be based on the patient’s risk level, skin condition, mobility, comfort, support surface, and care plan. Many bedridden patients need consistent position changes, but a universal schedule is not appropriate for everyone. A clinician or care team can help determine the safest routine. Caregivers should also watch for redness, discoloration, heel pressure, sliding, moisture, pain, or new skin changes between repositioning times.
How do wheelchair users prevent pressure sores?
Wheelchair users can reduce pressure sore risk through regular skin checks, weight shifts, posture review, properly fitted wheelchair cushions, foot positioning, moisture control, and breaks from prolonged sitting when appropriate. The cushion should match the person’s risk level, body shape, posture needs, and sitting time. Caregivers should watch the buttocks, sacrum, tailbone, back of thighs, and heels for discoloration, pain, warmth, or skin changes.
How can caregivers protect the tailbone?
Caregivers can help protect the tailbone by reducing prolonged pressure, reviewing sitting and lying positions, preventing sliding down in bed, checking skin daily, managing moisture, and using appropriate support surfaces when needed. For wheelchair users, cushion fit, posture, and sitting time matter. For bedridden patients, repositioning and mattress support matter. Tailbone redness or discoloration that does not fade should be monitored closely and discussed with a clinician.
How can caregivers protect heels?
Heel protection starts with daily skin checks, reducing direct pressure, managing moisture, and following the care team’s positioning guidance. Heels are vulnerable because they can press into the mattress for long periods. Some patients may need heel offloading, positioning supports, or a pressure redistribution surface. Caregivers should seek medical guidance if heel redness, dark discoloration, warmth, pain, blistering, open skin, drainage, or blackened tissue appears.
Does moisture increase pressure ulcer risk?
Yes. Moisture can weaken the skin and make it more vulnerable to friction, shear, and breakdown. Urine, stool, sweat, wound drainage, or damp bedding can soften skin and increase pressure injury risk, especially in patients with limited mobility or incontinence. Moisture management may include timely cleansing, changing damp clothing or bedding, using barrier products if recommended, and checking skin folds, buttocks, sacrum, and other high-risk areas consistently.
Does nutrition matter for pressure ulcer prevention?
Nutrition matters because skin needs enough calories, protein, fluids, vitamins, and overall nourishment to stay resilient and support healing. Poor appetite, weight loss, dehydration, illness, or low protein intake may increase vulnerability to skin breakdown. Caregivers should raise nutrition concerns with healthcare providers, especially if the patient is losing weight, eating poorly, recovering from illness, has wounds, or has repeated pressure injury risk.
Can movement help prevent bed sores?
Yes. Safe movement can help reduce prolonged pressure and improve comfort. Movement may include turning in bed, shifting weight while seated, standing briefly if safe, adjusting posture, therapy-guided activity, or caregiver-assisted repositioning. Even small changes can reduce pressure on the same skin area. Movement should match the patient’s strength, balance, medical condition, and care plan, especially after surgery, stroke, hospitalization, or major mobility decline.
How do you prevent skin breakdown during transfers?
Skin breakdown during transfers can be reduced by avoiding dragging, reducing friction, limiting shear, using proper technique, and using transfer aids or patient lifts when appropriate. Sliding across sheets, wheelchair fabric, or transfer surfaces can weaken skin. Caregivers should move slowly, protect bony areas, keep skin dry, use recommended equipment, and ask for training when transfers become difficult or unsafe for the patient or caregiver.
What should be included in a pressure ulcer prevention checklist?
A pressure ulcer prevention checklist should include daily skin checks, high-risk pressure points, repositioning according to the care plan, moisture control, bedding and clothing checks, nutrition and hydration monitoring, mattress and cushion review, safe transfer practices, mobility encouragement when possible, and a reporting plan for new redness, discoloration, warmth, pain, swelling, drainage, odor, blistering, or open skin. The checklist should be easy for caregivers to use consistently.
Mattresses, Cushions and Equipment
What mattress helps prevent bed sores?
The right mattress depends on the patient’s risk level, weight, mobility, moisture concerns, skin condition, and ability to reposition. Foam pressure redistribution mattresses may help lower to moderate risk patients. Alternating pressure systems may be considered for patients who spend long hours in bed and cannot reposition easily. Low air loss mattresses may help when heat and moisture are part of the care concern. A clinician can help match support surface to risk.
What is a pressure relief mattress?
A pressure relief mattress is designed to help reduce concentrated pressure on vulnerable areas such as the tailbone, hips, shoulders, and heels. Some mattresses redistribute pressure through foam or specialized surfaces, while others use air cells to shift pressure dynamically. Pressure relief mattresses can support a prevention plan, but they do not replace repositioning, skin checks, moisture control, nutrition, and medical guidance.
What is an alternating pressure mattress?
An alternating pressure mattress uses air cells that inflate and deflate in cycles to shift pressure across different parts of the body. These systems may be considered for patients with prolonged bed rest, limited ability to reposition, elevated pressure injury risk, or recurring skin concerns. They are part of a broader prevention plan and should be selected based on patient risk, comfort, wound status, and clinical guidance.
What is a low air loss mattress?
A low air loss mattress is designed to help with pressure redistribution and microclimate management by allowing airflow through the support surface. This may help manage heat and moisture around the skin. Low air loss systems are often considered for higher-risk patients, patients with moisture concerns, or more advanced care settings. They should be used as part of a full care plan that includes repositioning, skin checks, nutrition, and medical oversight.
Are foam mattresses useful for pressure relief?
Foam mattresses can be useful for pressure redistribution, especially for lower to moderate risk patients or prevention-focused care. They may help spread body weight more evenly and reduce concentrated pressure over bony areas. However, foam is not the right solution for every patient. Higher-risk patients, patients with recurring wounds, moisture concerns, or limited repositioning ability may need a more advanced support surface based on clinical guidance.
What wheelchair cushion helps with pressure relief?
A wheelchair pressure relief cushion should match the user’s pressure risk, posture, body shape, sitting time, sensation, and ability to shift weight. Foam cushions may support lower-risk users. Gel cushions may help with comfort and seated pressure distribution. Air cushions may provide adjustable pressure redistribution. Hybrid cushions combine materials for balance, stability, and comfort. Cushion fit is important because the wrong cushion can still allow pressure concentration.
Are gel cushions good for pressure sores?
Gel cushions may help with seated comfort and pressure distribution for some wheelchair users. They are often used when the concern is buttock pressure, tailbone discomfort, or long sitting periods. However, a gel cushion is not automatically the best choice for every pressure sore risk. Cushion selection should consider skin condition, posture, sensation, weight, chair fit, sitting time, and whether the user can perform weight shifts.
Are air cushions better for pressure relief?
Air cushions can provide adjustable pressure redistribution and may be helpful for higher-risk wheelchair users when properly selected, adjusted, and maintained. However, they are not always “better” for every person. Some users need more stability, posture support, or simpler maintenance. Air cushion performance can depend on correct inflation, fit, and user needs. A seating professional or clinician can help determine whether air, gel, foam, or hybrid cushioning is most appropriate.
Can a mattress prevent bed sores by itself?
No. A mattress can help reduce or redistribute pressure, but it cannot replace the full prevention routine. Bed sore prevention also requires repositioning, daily skin checks, moisture control, nutrition, hydration, safe transfers, activity when possible, and medical guidance. Even advanced surfaces need caregiver attention. If a patient is high risk, has open skin, or develops new discoloration, the care plan should be reviewed.
When should a caregiver consider a different mattress or cushion?
A caregiver may need to review the mattress or cushion when the patient develops redness, discoloration, pain, recurring pressure areas, heel concerns, buttock soreness, sliding, poor posture, increased time in bed, increased wheelchair sitting, moisture problems, or reduced ability to reposition. A worn mattress or cushion may also lose support. Equipment changes should be considered alongside the care plan, skin checks, repositioning, and clinical guidance.
Nursing Homes and Facilities
How do nursing homes prevent pressure ulcers?
Nursing homes help prevent pressure ulcers through admission skin assessments, routine skin checks, risk screening, repositioning plans, moisture management, nutrition monitoring, staff training, documentation, support surface planning, wheelchair seating review, and escalation when skin changes appear. A strong program turns risk identification into daily care. Families can ask how often skin is checked, how repositioning is documented, and how staff respond to redness or skin breakdown.
Are pressure ulcers a nursing home quality concern?
Yes. Pressure ulcers are a major quality and patient safety concern in nursing homes because they can reflect mobility limitations, skin risk, care consistency, nutrition issues, moisture management, support surface planning, and documentation. Not every pressure injury is preventable, but facilities are expected to have systems for identifying risk, monitoring skin, repositioning residents, communicating changes, and escalating concerns. Families should ask about prevention protocols and quality monitoring.
What should families ask a nursing home about bed sore prevention?
Families can ask how the facility checks skin on admission, how often high-risk residents are monitored, how repositioning is documented, how wheelchair seating is reviewed, how moisture and incontinence are managed, what support surfaces are available, how nutrition concerns are handled, and when families are notified about skin changes. They can also ask who evaluates new redness, heel changes, buttock pressure, or open skin.
What should hospitals do to reduce pressure injuries?
Hospitals reduce pressure injuries through structured skin assessment, risk screening, interdisciplinary prevention planning, repositioning, support surface use, heel protection, moisture management, nutrition review, staff training, documentation, and communication during transfers or discharge. Hospitalized patients may be at higher risk because of illness, surgery, weakness, sedation, devices, or limited mobility. Prevention works best when nurses, aides, therapists, wound care teams, and discharge planners coordinate consistently.
Why are pressure ulcers important in long-term care?
Pressure ulcers are important in long-term care because residents may have advanced age, chronic illness, limited mobility, incontinence, malnutrition, poor circulation, wheelchair use, or prior wounds. A pressure injury can cause pain, infection risk, longer recovery, and increased care needs. Long-term care teams need prevention systems that include staff training, skin checks, repositioning documentation, support surfaces, wheelchair cushions, nutrition monitoring, and family communication.
Do assisted living residents need pressure ulcer prevention plans?
Some assisted living residents do need pressure ulcer prevention plans, especially if they have limited mobility, wheelchair use, incontinence, diabetes, poor circulation, prior pressure sores, poor nutrition, or difficulty changing position. Assisted living staff and families should watch for skin changes, encourage mobility when safe, manage moisture, review seating and bedding, and communicate concerns early. Residents with worsening mobility may need additional clinical or home health support.
How can facilities choose support surfaces?
Facilities should choose support surfaces based on resident risk level, weight, mobility, skin condition, moisture concerns, wound history, wheelchair use, bariatric needs, and care environment. Some residents may need foam redistribution mattresses, while others may need alternating pressure, low air loss, bariatric surfaces, wheelchair cushions, heel protection, or transfer support. Equipment should be part of a documented prevention plan, not a replacement for staffing and skin monitoring.
Why is documentation important in pressure injury prevention?
Documentation helps facilities track skin status, risk level, repositioning, moisture care, nutrition concerns, support surface use, wheelchair seating, staff actions, wound changes, clinical escalation, and family communication. Without documentation, prevention can become inconsistent across shifts. Good documentation helps care teams identify patterns, respond earlier, coordinate across departments, and show that prevention protocols are being followed. It also supports quality improvement and accountability.
Review the most important sections again:
Key Takeaways
- Bed sores and pressure ulcers usually develop from prolonged pressure, often over bony areas.
- Early signs may include redness, discoloration, warmth, pain, swelling, or skin texture changes.
- High-risk patients include bedridden patients, wheelchair users, people with diabetes, stroke recovery patients, and nursing home residents.
- Prevention requires daily routines, not one single product.
- Repositioning, skin checks, moisture control, nutrition, mobility, and support surfaces all matter.
- Mattresses and cushions can help reduce pressure, but they do not replace caregiver attention or medical guidance.
- Facilities need prevention systems, staff training, documentation, and proper support surfaces.
Helpful Resources
Bed Sore Prevention Checklist
Printable checklist for daily skin checks, repositioning, moisture control, nutrition, mobility, and pressure relief routines.
Download the Bed Sore Prevention ChecklistHospital Bed Mattress Guide
Plain-language guide to hospital bed mattress types, support surfaces, pressure redistribution, and home care needs.
Read the hospital bed mattress guideBest-Selling Hospital Bed Mattresses
Compare popular mattress options for comfort, pressure support, home care, and long-term patient needs.
Compare best-selling hospital bed mattressesHospital Bed Mattress FAQs
Answers to common caregiver questions about mattress terms, support types, sizing, and pressure relief options.
Review hospital bed mattress FAQsWheelchair Seat Cushion Guide
Learn how foam, gel, air, and hybrid cushions support comfort, posture, pressure relief, and seated skin protection.
Read the wheelchair cushion guideWheelchair Seat Cushions
Explore wheelchair cushion options for comfort, positioning, pressure redistribution, and seated support.
View wheelchair seat cushionsAging in Place Statistics Report
Research-based report on home care, senior safety, aging in place, and the growing need for safer care environments.
Read the aging in place statistics reportElderly Fall Statistics Report
Patient safety report covering elderly fall data, hospital risks, nursing home safety, and prevention insights.
Read the elderly fall statistics reportFinal Patient Safety Reminder
Preventing pressure ulcers starts with awareness, early skin checks, consistent repositioning, and the right care environment. For families, caregivers, and facilities, the goal is not only to treat wounds after they appear — it is to reduce the conditions that allow skin breakdown to begin.
About the Author
Pinny Surkis is the Founder of MedCare Mobility, a national provider and authorized dealer of premium home medical equipment. He researches patient transfers, Hoyer lifts, patient lift slings, pressure relief mattresses, mobility solutions, and caregiver safety while developing educational resources that help patients, families, caregivers, and healthcare professionals make more informed equipment decisions.
Learn More About Pinny Surkis and His Research

