
Why Seniors Prefer Home
Home offers familiarity, privacy, personal control, emotional comfort, and closer family and community connections.

Jun
Aging in place means remaining safely and comfortably in your own home as you grow older instead of moving directly into assisted living or nursing home care. This report brings together aging in place statistics, aging in place trends, home care statistics, caregiver challenges, and home safety research to help families plan for safer independent living.
Aging in place is the ability of an older adult to continue living safely, independently, and comfortably in a familiar home while receiving the mobility assistance, caregiver help, home modifications, and healthcare support needed as their needs change.
For many families, the question is not simply whether a senior wants to remain at home. It is whether the home, care plan, and available support can safely address fall risk, mobility decline, chronic conditions, daily activities, and caregiver demands.
Home offers familiarity, privacy, personal control, emotional comfort, and closer family and community connections.
Falls, mobility decline, hospitalization, unsafe rooms, chronic illness, and limited caregiver support can make living at home more difficult.
Successful aging in place often requires early home safety planning, caregiver coordination, mobility support, and regular reassessment.
Use these printable tools to review safety, mobility, caregiver needs, and aging in place readiness.
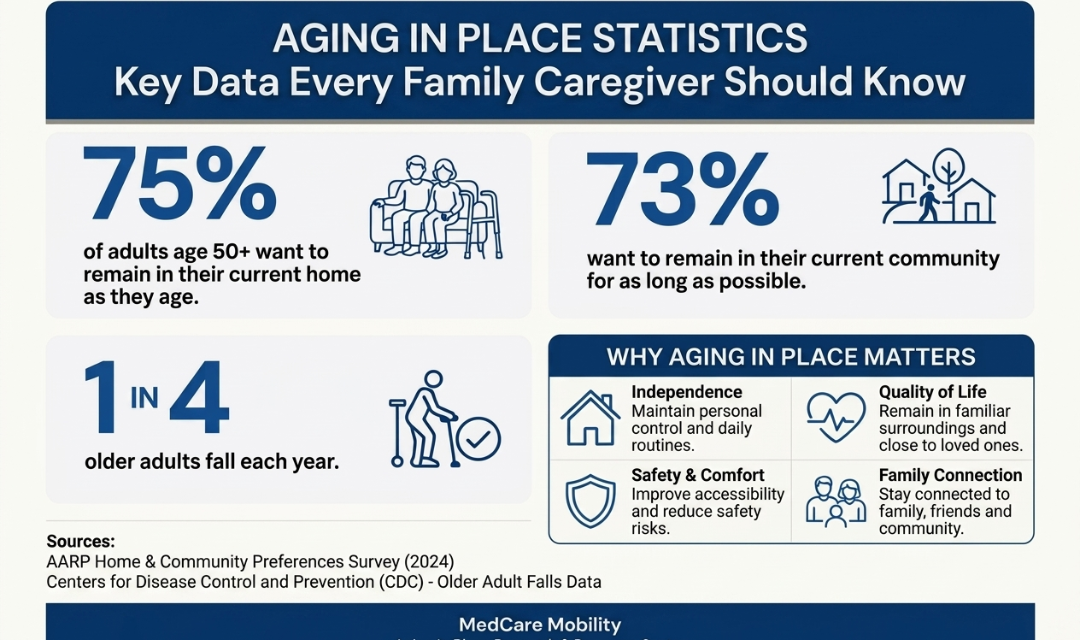
Introductory data: AARP Home & Community Preferences Survey and CDC Older Adult Falls Data.
Aging in place statistics show a clear national shift toward home-based care, family caregiving, senior home safety planning, and long-term independence. The numbers matter because they explain why more families are preparing homes before a health event, fall, hospitalization, or mobility decline forces a sudden decision.
The strongest aging in place trend is not simply that older adults prefer home. It is that families are increasingly trying to make the home safer, more accessible, and more realistic for changing care needs. This includes planning for fall prevention, bathroom safety, bedroom safety, caregiver support, mobility changes, and home care services.
As the senior population grows, aging in place data is becoming more important for adult children, caregivers, healthcare providers, discharge planners, and older adults themselves. A safe home care plan must account for independence, daily routines, medical needs, physical limitations, and the ability of caregivers to help without becoming overwhelmed.

More families are exploring home care services, private caregiving, daily living assistance, and home-based support before considering assisted living or nursing home care.
As the older adult population increases, more homes will need to be prepared for mobility changes, chronic conditions, fall prevention, and long-term care needs.
Family caregivers often become the foundation of aging in place, helping with transfers, meals, medication reminders, bathing, dressing, and safety monitoring.
Successful aging in place usually requires planning before a crisis, especially when fall risk, weakness, stairs, unsafe bathrooms, or caregiver strain are already present.
Together, these aging in place trends show why home safety for seniors, caregiver planning, senior mobility support, and home accessibility are no longer optional topics. They are part of how families protect independence, reduce avoidable injury risks, and make home-based care more sustainable.
Most older adults do not want institutional care. They want to remain independent, connected to family, and safe at home for as long as possible.
Source areas referenced for this section include CDC Older Adult Falls Data, AARP Home & Community Preferences research, the Administration for Community Living, the National Institute on Aging, and the U.S. Census Bureau.
Seniors often lose independence gradually, then suddenly. A small change in balance, strength, memory, mobility, or caregiver support can make everyday activities harder and increase the risk of falls, hospitalization, or the need for facility-based care.

For many older adults, independence is affected by a chain reaction. A fall can lead to fear of falling. Fear can lead to less walking. Less walking can lead to weakness, balance decline, and greater dependence on caregivers. Over time, the home that once felt safe may become difficult to navigate.
This is why aging in place planning must look beyond basic comfort. Families need to understand the most common independence risks before they become emergencies.
Falls are one of the biggest threats to senior independence. Even when a fall does not cause a major injury, fear of falling can reduce confidence, movement, and daily activity.
Weakness, poor balance, pain, and reduced endurance can make it difficult to walk safely, get out of bed, rise from a chair, or move around the home.
Stroke, Parkinson’s disease, neuropathy, and other neurological conditions may affect strength, coordination, walking ability, transfers, and daily care routines.
Arthritis can make standing, walking, gripping, bathing, dressing, and repositioning more difficult, especially when pain limits movement throughout the day.
After a hospital stay, seniors may return home weaker, less steady, or more dependent than before, making discharge planning and home safety preparation especially important.
When transfers, repositioning, bathing, or toileting become too physically demanding, caregivers may struggle to provide safe help without equipment or additional support.
The loss of independence is rarely caused by one problem alone. It often comes from the combination of physical decline, unsafe home layouts, chronic conditions, caregiver strain, and delayed planning. Families who identify these risks early can often make the home safer and reduce avoidable emergencies.
Falls remain one of the leading causes of injury, hospitalization, and loss of independence among older adults.
Source areas referenced for this section include CDC fall prevention resources, the National Institute on Aging, the Administration for Community Living, and NIH research related to mobility, aging, chronic conditions, and senior independence.
Aging in place often depends on family caregivers, but many caregivers are asked to manage physical care, emotional support, transportation, medication reminders, transfers, household tasks, and safety monitoring without enough training, equipment, or backup support.
Family caregiver statistics show why caregiver support is such an important part of aging in place planning. When an older adult begins needing help with bathing, toileting, dressing, getting out of bed, walking, or transferring from one surface to another, the responsibility often falls on a spouse, adult child, or relative.
Over time, this can create serious caregiver stress. Many families start with small tasks and gradually move into high-risk physical assistance, including lifting, repositioning, and transfers. Without the right plan, caregiver burnout, back strain, sleep disruption, and emotional fatigue can make home care harder to sustain.
These signs may indicate that the current home care plan needs more support, safer equipment, or additional help.
Lifting, pulling, repositioning, and helping with transfers can place major strain on a caregiver’s back, shoulders, knees, and wrists.
Bed-to-chair, wheelchair-to-toilet, and chair-to-standing transfers can become unsafe when the senior cannot reliably bear weight.
Overnight bathroom needs, repositioning, pain, confusion, or fall concerns can leave caregivers exhausted and less able to provide safe care.
Watching a loved one decline while managing daily care decisions can create stress, guilt, frustration, and decision fatigue.
Caregiver burnout statistics are important because aging in place is not only about the senior’s needs. It is also about whether the caregiver can safely continue helping. A home care plan that ignores caregiver strain may eventually lead to emergency falls, unsafe transfers, preventable injuries, or the need for a higher level of care.
Millions of family caregivers provide unpaid assistance every year, often while balancing careers, families, and their own health concerns.
Source areas referenced for this section include caregiver research from national aging, health, and public health organizations, including resources related to family caregiving, caregiver stress, safe patient handling, and aging in place support.
The financial side of aging in place is one of the biggest reasons families begin researching home care statistics, senior safety planning, and long-term care options. The true cost of aging is not only the monthly price of care. It also includes hidden expenses, caregiver time, home modifications, medical equipment, transportation, and the impact of preventable falls or hospitalizations.
Families often compare aging in place, assisted living, and nursing home care as if they are simple monthly costs. In reality, each option has different tradeoffs. Aging in place may require home safety upgrades, caregiver support, mobility equipment, and home care services, while facility-based care may include higher monthly housing and care costs.
The most important question is not only “Which option costs less?” It is “Which option is safest, most realistic, and most sustainable for the senior and the caregiver?” A lower-cost plan can become expensive if it leads to falls, caregiver injuries, repeated hospital visits, or unsafe transfers.

| Care Option | Common Costs | Hidden Costs | Planning Considerations |
|---|---|---|---|
| Aging In Place | Home care services, medical equipment, home safety modifications, transportation, caregiver support. | Unpaid caregiver time, missed work, home repairs, emergency fall risks, added help after hospitalization. | Best when the home can be made safe and caregiver support is realistic, consistent, and sustainable. |
| Assisted Living | Monthly residence fees, personal care assistance, meals, activities, medication support, added care levels. | Move-in fees, care-level increases, transportation, private aides, supplies, and services not included in base pricing. | May help when daily supervision is needed but skilled nursing care is not yet required. |
| Nursing Home Care | Room, meals, skilled nursing care, assistance with daily living, clinical monitoring, rehabilitation support. | Long-term financial impact, eligibility rules, private-pay periods, personal items, and transition costs. | Often considered when medical needs, mobility limitations, or safety risks exceed what can be managed at home. |
Home care may include hourly aides, family caregiver support, safety equipment, home modifications, transportation, and daily living assistance.
Assisted living and nursing home costs can vary widely depending on location, care level, room type, and whether skilled care is required.
Unpaid caregiving can still carry a financial cost through lost work hours, physical strain, emotional stress, and reduced personal time.
The strongest plan looks beyond today’s expenses and prepares for mobility decline, fall risk, discharge needs, and caregiver limits.
For families comparing aging in place costs with assisted living or nursing home care, the goal should be realistic planning. A safe home may require upfront investment, but the right support can help reduce fall risks, ease caregiver strain, delay unnecessary facility placement, and preserve independence longer.
For many families, aging in place can preserve independence and quality of life while delaying or avoiding higher-cost institutional care.
Source areas referenced for this section include Genworth Cost of Care research, CMS, Medicare long-term care information, and Administration for Community Living resources related to aging, caregiving, and long-term support planning.
Home safety is one of the most important parts of aging in place. Many senior falls happen during normal daily routines, including getting out of bed, walking to the bathroom, standing from a chair, using stairs, entering the home, or moving through poorly lit rooms.
A safe aging in place plan should review the home room by room. The goal is not only to remove obvious hazards, but to understand where the senior is most likely to lose balance, become fatigued, need help, or rely on unsafe furniture for support.
Home safety for seniors often includes fall prevention, better lighting, safer pathways, bathroom accessibility, bedroom setup, mobility planning, and caregiver support. Small changes can make a major difference when they are made before a fall or hospitalization occurs.
Low beds, unstable nightstands, loose rugs, poor lighting, and difficult transfers can increase fall risk during nighttime routines.
Wet floors, low toilets, tubs, narrow spaces, and lack of grab support can make bathrooms one of the highest-risk areas in the home.
Soft chairs, clutter, cords, throw rugs, low seating, and unstable furniture can make sitting, standing, and walking more difficult.
Dim hallways, dark bathrooms, glare, shadows, and poor nighttime visibility can increase the chance of slips, trips, and missteps.
Steps, thresholds, uneven walkways, missing handrails, and outdoor entry points should be reviewed before mobility declines further.
Walkers, rollators, wheelchairs, transfer help, and safer room layouts should match the senior’s current strength and balance level.
| Home Area | Common Risk | Warning Signs | Planning Action |
|---|---|---|---|
| Bedroom | Difficult bed transfers, poor nighttime visibility, unstable furniture, clutter near walking paths. | Struggling to sit up, sliding in bed, reaching for furniture, needing help overnight. | Review bed height, lighting, bedside access, support rails, repositioning needs, and caregiver safety. |
| Bathroom | Wet floors, tub transfers, low toilet height, lack of support, narrow movement space. | Fear of bathing, near-falls, difficulty standing from the toilet, needing hands-on help. | Assess grab support, toileting support, shower access, non-slip surfaces, and transfer assistance. |
| Living Room | Low chairs, soft seating, throw rugs, cords, crowded furniture, poor walking paths. | Rocking to stand, pushing on unstable furniture, shuffling, avoiding certain areas. | Improve seating height, clear pathways, remove trip hazards, and match mobility equipment to the room layout. |
| Stairs & Entrances | Uneven steps, thresholds, missing railings, poor outdoor lighting, slippery entry areas. | Holding walls, avoiding stairs, needing help entering the home, fatigue after short distances. | Review handrails, ramps, threshold transitions, entry lighting, and whether the main living area should be reconfigured. |
Many falls are preventable through simple modifications, mobility support equipment, proper lighting, and proactive planning.
Source areas referenced for this section include fall prevention, aging in place, home safety, and older adult mobility guidance from national public health and aging organizations.
Home care equipment should never replace proper medical advice, caregiver planning, or home safety evaluation. However, the right equipment can make aging in place more realistic by helping seniors move more safely, rest more comfortably, reduce pressure injury risks, and lower the physical strain placed on family caregivers.
This is where aging in place planning becomes practical. Once families understand the risks — falls, mobility decline, caregiver strain, unsafe rooms, and hospitalization — they can begin matching the home environment to the senior’s daily needs. The goal is not to buy equipment randomly. The goal is to identify which tools support safer movement, better positioning, easier transfers, and greater independence.
Home care solutions should be chosen based on the senior’s mobility level, transfer ability, balance, skin health, caregiver support, room layout, and long-term care plan.
A hospital bed can support safer positioning, easier caregiving, better transfers, and improved comfort for seniors who spend significant time in bed.
Patient lifts may help when transfers become unsafe, especially if a senior cannot reliably stand, pivot, or bear weight without assistance.
Medical mattresses can support pressure relief, comfort, moisture management, and skin protection for seniors with limited mobility.
Walkers and rollators can help seniors maintain movement, reduce fall risk, and improve confidence when walking around the home or community.
Wheelchairs can support safer mobility when walking becomes limited, tiring, painful, or unsafe for longer distances.
The best home care equipment is chosen around a real need. A person who mainly struggles with balance may need a walker or rollator. A person who cannot safely transfer may need a patient lift. A person who spends long hours in bed may need a better mattress, safer positioning, or a hospital bed setup. Matching the solution to the problem is what makes equipment useful.
The right mobility and safety equipment can significantly reduce fall risks, ease caregiver strain, and help seniors remain independent longer.
This section is intended for educational planning only. Families should consider the senior’s medical condition, mobility level, caregiver support, and professional recommendations when choosing home care equipment.
The central message of this aging in place report is simple: remaining at home is not only a preference. It is a safety, caregiving, mobility, financial, and planning challenge that must be prepared for before a crisis happens.
Families should treat aging in place as a long-term care plan, not a one-time decision. Review fall risks, bedroom setup, bathroom safety, caregiver capacity, mobility changes, and emergency plans before the senior’s needs become urgent.
Caregivers need protection too. If transfers, repositioning, toileting, bathing, or nighttime care are becoming physically difficult, the care plan may need equipment, outside help, or a safer transfer strategy.
Discharge planning and senior care planning should include home safety, caregiver readiness, fall prevention, mobility support, and whether the patient can safely perform daily activities at home.
Aging in place is about preserving independence, dignity, routine, and community connection. The safest plans support confidence while reducing preventable risks inside the home.
Use these printable resources to turn the report into a practical home safety and care planning review.
As the older adult population grows, aging in place will become an even more important part of home care, caregiver support, senior mobility, and fall prevention planning. Families who prepare early are often better positioned to protect independence, reduce preventable risks, and support quality of life over the long term.
These aging in place FAQs answer common questions families, caregivers, older adults, discharge planners, and home care decision-makers ask when planning for senior safety, independence, mobility, caregiving, and long-term care at home.
Aging in place means an older adult continues living safely, independently, and comfortably in their own home or community as they age, instead of moving directly into assisted living or nursing home care. Successful aging in place usually requires home safety planning, caregiver support, mobility planning, and regular reassessment as needs change.
A large majority of older adults say they want to remain in their homes or communities as they age. The key issue is not only preference, but whether the home environment, caregiver support, mobility level, and safety plan can realistically support independent living over time.
Older adults often prefer aging in place because home provides familiarity, privacy, routine, emotional comfort, independence, and connection to family and community. For many seniors, staying at home also helps preserve dignity and control over daily life.
The main benefits of aging in place include independence, familiar surroundings, emotional comfort, family connection, personalized routines, and the possibility of delaying facility-based care. These benefits are strongest when the home is safe and the care plan matches the senior’s actual needs.
Aging in place can improve quality of life when the senior can remain safe, supported, socially connected, and comfortable at home. However, quality of life may decline if the home is unsafe, caregiving is overwhelmed, mobility is poor, or the senior is isolated without enough support.
Families should begin aging in place planning before a crisis occurs, ideally when the older adult is still relatively independent. Planning early makes it easier to identify fall risks, home modifications, caregiver needs, mobility changes, and future equipment needs before an emergency fall or hospital discharge forces rushed decisions.
The biggest risks to independent living include falls, mobility decline, weakness, chronic illness, cognitive changes, unsafe bathrooms, poor lighting, stairs, hospitalization, and limited caregiver support. These risks often overlap and can quickly make daily activities harder.
Seniors often lose independence because of falls, fear of falling, reduced strength, balance problems, stroke, arthritis, neurological disease, hospitalization, memory changes, or caregiver limitations. Loss of independence is usually a gradual pattern that becomes more serious when risks are not addressed early.
Falls are very common among older adults and are one of the leading safety concerns for seniors aging at home. A fall can cause injury, reduce confidence, increase fear, and lead to less activity, which may further weaken balance and mobility.
Falls are one of the leading causes of injury among older adults. They can result in fractures, head injuries, hospitalization, reduced confidence, loss of mobility, and a higher need for caregiving or facility-based care.
Warning signs include repeated falls or near-falls, trouble getting out of bed or chairs, unsafe bathroom transfers, missed medications, poor hygiene, confusion, weight loss, isolation, caregiver exhaustion, and difficulty walking through the home safely.
Your parent may be able to remain safely at home if they can move through the home, bathe, toilet, transfer, eat, take medications, and get help when needed without major risk. If they need frequent hands-on assistance, have repeated falls, or the caregiver is overwhelmed, the home care plan should be reassessed.
Helpful home modifications may include better lighting, clear walking paths, grab bars, non-slip bathroom surfaces, safer seating, bed-height adjustments, removal of throw rugs, threshold changes, handrails, ramps, and keeping daily essentials within easy reach.
The most important aging in place safety tips are to prevent falls, improve bathroom safety, brighten dark areas, remove trip hazards, review bed and chair transfers, match mobility equipment to the senior’s ability, support caregivers, and reassess the home whenever health or mobility changes.
Caregiver burnout is physical, emotional, and mental exhaustion caused by ongoing caregiving demands. It can happen when a caregiver is responsible for transfers, bathing, toileting, medication reminders, household tasks, supervision, and emotional support without enough rest or backup help.
Caregiver stress is very common, especially among family caregivers who provide unpaid help while also managing work, children, finances, and their own health. Stress increases when the older adult needs physical lifting, nighttime care, supervision, or frequent hands-on assistance.
Signs of caregiver burnout include exhaustion, poor sleep, irritability, anxiety, sadness, back pain, missed personal appointments, resentment, isolation, and feeling unable to continue providing safe care. Burnout should be treated as a care planning issue, not a personal failure.
Caregivers can reduce physical strain by avoiding manual lifting when possible, using proper transfer techniques, clearing pathways, adjusting bed and chair height, using mobility aids when appropriate, and considering patient lifts or transfer equipment when standing and pivoting become unsafe.
Families can support a caregiver by sharing responsibilities, arranging respite care, helping with transportation and meals, reviewing home safety, providing backup coverage, reducing unsafe lifting tasks, and listening when the caregiver says the current plan is becoming too difficult.
Families should seek additional help when the senior needs frequent transfers, bathing support, toileting assistance, overnight supervision, medication reminders, fall monitoring, or care that is physically or emotionally overwhelming for the family caregiver.
Aging in place may be less expensive than assisted living for some families, especially when care needs are limited. However, costs can rise with paid home care, safety modifications, medical equipment, transportation, and caregiver time. The safest comparison includes both visible and hidden costs.
Aging in place may cost less than nursing home care when medical needs are manageable at home. But if the senior needs 24-hour care, complex medical support, frequent transfers, or constant supervision, home care costs can increase significantly.
Hidden aging in place costs may include unpaid caregiver time, missed work, home modifications, emergency repairs, transportation, medical supplies, equipment, paid aides, fall-related expenses, and extra help after hospitalization.
Families can prepare financially by estimating home care needs, reviewing insurance coverage, planning for equipment and modifications, comparing care options, discussing caregiver availability, and creating a plan for how needs may change after a fall, illness, or hospital stay.
An aging in place checklist usually includes home safety, fall risks, bathroom setup, bedroom safety, lighting, mobility needs, caregiver support, emergency planning, medication routines, accessibility, financial planning, and equipment needs.
Seniors often move into assisted living or nursing homes when daily care needs become too difficult or unsafe to manage at home. Common reasons include falls, mobility decline, cognitive changes, hospitalization, caregiver burnout, inability to perform daily activities, and lack of reliable support.
Equipment that may help seniors stay independent includes walkers, rollators, wheelchairs, hospital beds, medical mattresses, lift chairs, bedside tables, bathroom safety equipment, trapeze bars, transfer aids, and patient lifts. The right equipment depends on the senior’s mobility, balance, caregiver support, and home layout.
A patient lift should be considered when an older adult cannot safely stand, pivot, or transfer with normal assistance, or when caregivers are physically lifting and risking injury. Patient lifts are often used for bed-to-wheelchair, wheelchair-to-chair, and toileting-related transfers when manual transfers become unsafe.
A hospital bed may be considered when a senior needs frequent repositioning, safer bed height, head or leg elevation, easier caregiving, pressure relief support, or help getting in and out of bed. It may also help after hospitalization or when mobility declines.
Mobility equipment that may reduce caregiver strain includes walkers, rollators, wheelchairs, transfer aids, patient lifts, hospital beds, trapeze bars, and lift chairs. These tools can reduce unsafe pulling, lifting, bending, and repositioning when matched correctly to the senior’s needs.
Common medical equipment for aging in place includes walkers, rollators, wheelchairs, shower chairs, grab bars, hospital beds, pressure relief mattresses, bedside commodes, lift chairs, trapeze bars, overbed tables, and patient lifts.
Use the resources below to continue planning safer aging in place, compare home medical equipment options, and review practical guides for mobility, transfers, pressure relief, fall prevention, and caregiver support.
Pinny Surkis is the Founder of MedCare Mobility, a national provider and authorized dealer of premium home medical equipment. He researches patient transfers, Hoyer lifts, patient lift slings, pressure relief mattresses, mobility solutions, and caregiver safety while developing educational resources that help patients, families, caregivers, and healthcare professionals make more informed equipment decisions.
Learn More About Pinny Surkis and His Research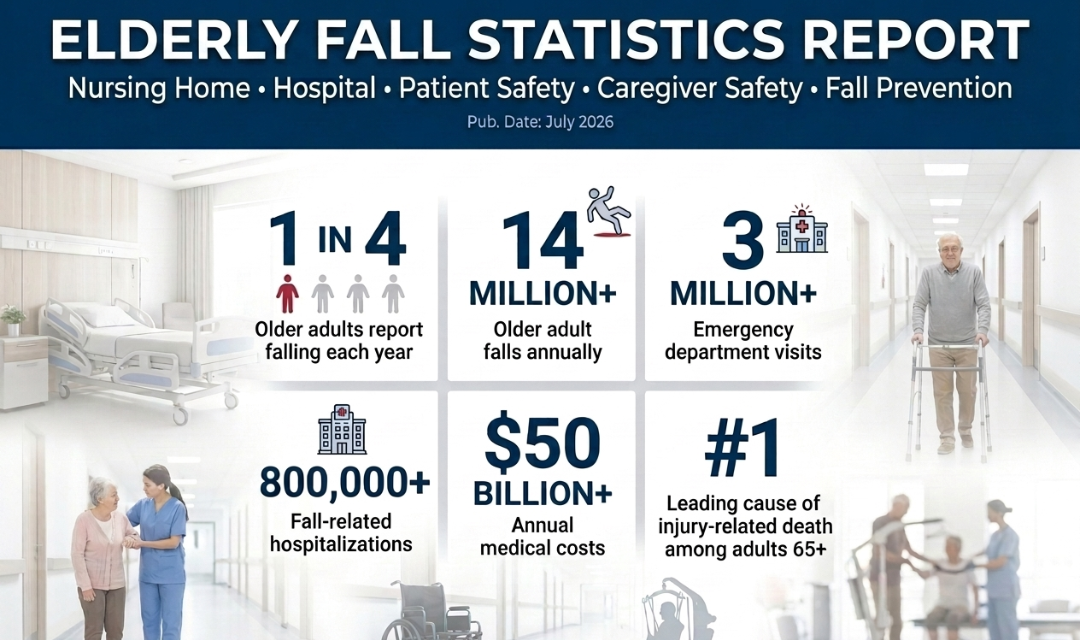
Successful aging in place depends on preparation, not hope.
Most older adults want to remain at home, but the ability to age in place safely depends on whether the home, caregiver support system, mobility plan, and daily care setup can adapt as needs change. Falls, hospitalization, weakness, caregiver burnout, pressure injury risk, unsafe bathrooms, and poor transfer planning are often connected. One problem can quickly create another.
Families should not wait until a fall, discharge, caregiver injury, or sudden decline forces an urgent decision. The strongest aging in place plans begin early, review risks honestly, and match support to the person’s actual daily function.